NPC Comments on Public Request for Input on Cures 2.0
December 16, 2019
The Honorable Diana DeGette
2111 Rayburn House Office Building
Washington, DC 20515
The Honorable Fred Upton
2183 Rayburn House Office Building
Washington, DC 20515
Submitted electronically via [email protected]
Dear Representative DeGette and Representative Upton,
Thank you for the opportunity to submit comments on a second iteration of the 21st Century Cures Act. The National Pharmaceutical Council (NPC) shares your goal of modernizing coverage and access to life-saving cures.
NPC is a health policy research organization dedicated to the advancement of good evidence and science and to fostering an environment in the United States that supports medical innovation. NPC is supported by the major U.S. research-based biopharmaceutical companies. We focus on research development, information dissemination, education and communication of the critical issues of evidence, innovation and the value of medicines for patients. Our research helps inform important health care policy debates and supports the achievement of the best patient outcomes in the most efficient way possible.
Our comments today will focus on the following topics:
- Expediting coverage for new medical products;
- Use of real-world evidence (RWE); and
- Incorporating the patient and caregiver voice.
Barriers to Implementation Need to be Addressed to Ensure Coverage and Access for Innovative New Therapies and Cures
The 21st Century Cures Act was designed to speed the approval of new drugs and boost funding for medical research. These efforts and others have seen the steady flow of new cures and treatments for devasting illness. However, with innovative breakthroughs comes concerns regarding cost, patient access and affordability. Added to that complexity is the intricate health care and payment system in the United States, impacted by the funding source (self-insured employers, commercial insurers, Medicaid and Medicare) goals and the of benefit designs, payment and coverage policies incentivizing treatment payment. Overlaying these challenges is the system transformation from a transactional health system that rewards volume and quantity to a system that focuses on the value that a product or procedure provides.
Innovative and durable treatments require new and multiple financing tools
While there have been efforts to incorporate more value into healthcare, there are barriers to this change that may ultimately limit access to new therapies. For example, with one-time treatments, the high upfront costs can be a major concern for some payers. For other treatments with high unmet needs and small patient populations, there may be uncertainty associated with the time of approval, administration and payment in any specific quarter or year. Finally, the cumulative impact of multiple treatments can raise concerns due to the number of treatments on the horizon and the member population in any quarter.
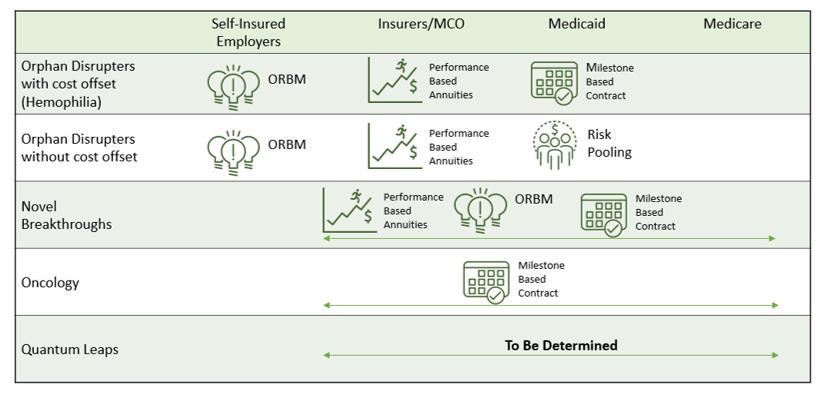
Despite these challenges, payors are interested in finding creative solutions to these innovations. Working to modernize access and coverage issues will require an understanding of the variable U.S. market, including what matters to each payer, including self-insured employers, commercial insurers, Medicare and Medicaid. Each of these payors is influenced differently by timing, therapeutic performance, actuarial risks,[1] and administrative and financial capacity. These varied interests mean that payors will need flexibility and multiple options as they seek to provide access and coverage for novel therapeutics. Several ideas have been explored, including:
- Milestone-based contracts
- Population risk pooling
- Annuities designed to spread payments over multiple years
- Performance-based annuities to spread out and tie payment to performance.[2]
The table below outlines how different payer segments may address new innovative therapies and cures.
Legislative and regulatory reforms are needed to enable new financing approaches
Even with interest from payers for new financing approaches, significant barriers to implementation remain. Without addressing these barriers, less than half of all plans cover durable cures and most frequently cover these treatments with more restrictions than the approved product label. Nearly four out of five payers rate their concern as “high” or “extremely high” due to the total cost to the plan, product performance and durability, actuarial risk, or payment timing relative to the realization of benefits. Regardless of the financing tools implemented, policy changes, operational capabilities and risk management approaches will be needed as outlined in the table below:
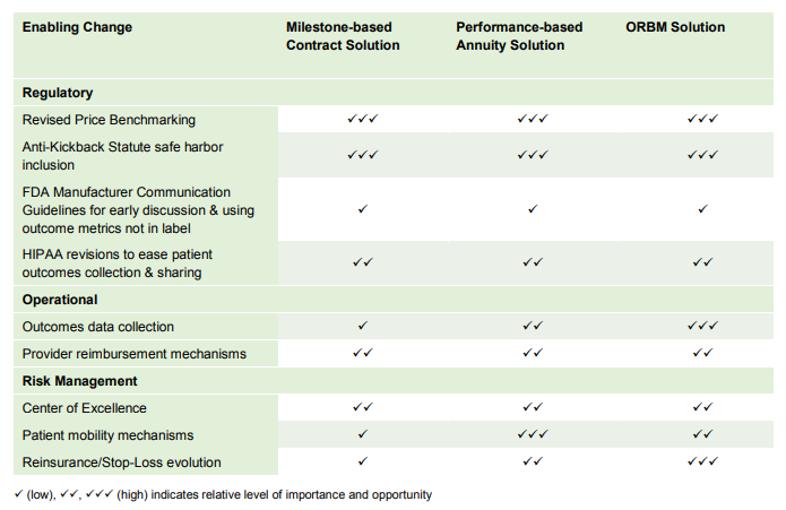
The ability to employ new financing tools is impacted by federal price benchmarks such as Medicaid Best Price regulations and 340B ceiling prices. However, these price benchmarks are not flexible enough to allow for new payment innovations such as performance-based or milestone-based contracts without profound downstream costs. Further, many durable treatments are inhaled, infused, instilled, implanted or injected and therefore fall into the 5i drugs included in the Average Manufacturer Price, which may impact prices substantially if alternative payment contracts exist. Finally, Average Sales Price or (ASP) includes performance payments, which may be highly volatile if only small patient populations are treated. Without regulatory exemptions, new financing tools for durable treatments and cures create risk for both payers and biopharmaceutical manufacturers.
Current benefit designs may limit access to new therapies
New innovative curative therapies and other single administration products present challenges for payors due to their unique set-up that may not neatly fit into the payment structures and incentives built into insurance benefits designs. Most insurance designs use deductibles and copays to reduce inappropriate use or over-use of routine therapies. Traditional benefit designs may have unintended consequences for new precision therapies that target selective populations or require one-time administration.[3] Many health plans have suggested waiving the prevailing patient coinsurance contribution as the optimal path forward for one-time administration products. However, this health plan waiver could trigger a state insurance review, which could take as long as 18 months.[4] Delaying treatment until the appropriate waiver is received could lead to even more significant health problems.
New payment approaches should use pilot programs to assess sustainability
As payors continue to work towards new strategies for covering new therapies, it will be important to consider and test methods before widespread implementation. Often, only small sample sizes will be associated with potential new cures, which can limit the exposure of both intended and unintended consequences. New coverage programs should be tested and evaluated through pilot programs first. Pilot programs and waivers allow payors, providers and patients to understand the impact and evaluate the suitability for relevant populations. Federal agencies need to have the flexibility to support pilot programs and other endeavors.
Use of Real-World Evidence (RWE) Should be Expanded
FDA RWE program needs a clear vision, transparent implementation timelines and a centralized repository of decisions and programs
The 21st Century Cures Act took great strides toward enhancing the use of real-world evidence by requiring the FDA to establish a program that evaluates the use of real-world evidence to support drug approvals. The FDA has begun this work, releasing the Framework for FDA’s Real-World Evidence Program[5] as well as guidance on how to submit RWE with drug applications.[6] While these were important first steps, NPC believes that additional steps can enhance the use of real-world evidence in developing and providing access to life-saving therapies.
To build upon the initial groundwork laid by 21st Century Cures and the FDA’s subsequent activity, a clear vision to advance the use of RWE should be defined. Accomplishing this will require accessible and interoperable data, trusted curation methods, credible analytics, new cutting-edge data skills and cultural adoption. Laying out the vision with clear objectives will be essential for stakeholders to contribute to this effort. Without clarity of the regulatory vision, the use of real-world data and RWE tools may be stymied. We believe it will be helpful for all stakeholders to understand the ultimate vision of the RWE Program as laid out by the FDA.
In addition, timelines for programmatic elements of the FDA’s RWE framework should be announced in advance to allow for external engagement. Delineation of the timetable for the programmatic elements and funded pilot programs provides interested researchers and stakeholders with ample opportunity to contribute research and set aside needed resources to provide input during future engagement opportunities. Further clarity on how public comments will be considered creates credibility and trust.
Finally, a centralized repository of all regulations, guidance and other documents surrounding RWE is needed. The FDA’s RWE Subcommittee of the Center for Drug Evaluation and Research (CDER) Medical Policy and Program Review Council will address cross-cutting issues. A central repository for guidance related to RWD and RWE would allow a complete view of these documents and their applicability in harnessing these tools to both those within and outside the government. In particular, a central repository would provide clarity to organizations interested in the criteria and standards for implementing RWE. NPC recommends this central repository to ensure a harmonized view of documents and enable a consistent application of RWE tools across divisions, regulatory decisions, and biopharmaceutical manufacturers.
NPC recommends outlining which regulatory decisions RWE may be useful in addressing, providing timelines for various programmatic elements, and offering opportunities for stakeholders to contribute and provide input. These efforts will ensure that the full potential of RWE — including post-market regulatory decisions — is realized.
RWE use in federal policy should expand beyond the FDA
The use of RWE by the FDA marks an important first step, but the use of RWE should be considered across federal health care programs and payment policies. Payment and coverage decisions are one area where RWE could be utilized. Many of these decisions for federal programs such as Medicare frequently focus on the evidence gathered from randomized controlled clinical trials (RCTs). While RCTs offer important insight into the efficacy of a drug, NPC believes that other types of evidence, in particular, real-world evidence (RWE), are appropriate for incorporation into coverage decisions.
Just as the FDA is evolving in its use of real-world data, we encourage CMS to adopt a similar stance on the broader use of real-world evidence and data in programs such as the New Technology Add-on Payments (NTAP). Clinical trial design can vary depending on the drug and affected patient population. For many populations and treatments, RWE may not be available until there is sufficient use. For orphan disease populations, historical or retrospective real-world data can be beneficial when there are few patients to sample from, or an RCT is not the most feasible or ethical design option. These retrospective studies or historical control arms are used to support regulatory approval or payment and coverage decisions. Furthermore, these studies can provide valuable insight into how a drug performs, particularly compared to past treatments. By considering this data and other real-world evidence, NPC believes CMS can further its goal of facilitating patient access to innovative technologies.
Beyond the FDA, other stakeholders are beginning to use RWE to understand how certain treatments work across care settings and more diverse populations. Real-world evidence can also be a useful tool as the health care environment shifts to a more value-based system with a focus on care coordination, quality of care, and risk-sharing.[7] In a payer roundtable convened by NPC, participants noted the value of RWE to fill in information gaps for payment and coverage.[8] Similarly, RWE can provide a deeper understanding of how certain patient populations that differ from clinical trials due to age, race or ethnicity are affected by a new innovative treatment in typical care settings.
Despite the potential for RWE to inform coverage, consistent use of evidence remains an aspiration. NPC research, in partnership with the researchers from Tufts Medical Center, found little consistency in the evidence commercial health plans reviewed when making specialty drug coverage policies. For example, the same study was cited in 15 percent of health plan coverage policies for a given drug and condition. The volume of evidence used to inform coverage decisions varied greatly, from an average of 4 studies cited in coverage decisions by one health plan to an average of 64 studies cited by another health plan. Even the breadth and types of clinical and economic evidence used to inform the coverage decisions varied; RWE was incorporated by some health plans and not considered by other health plans.[9] The reasons for such variation include limitations in the available evidence as well as lack of experience by health plan representatives and their organization interpreting and conducting such studies.[10]
Real-world evidence can provide valuable insights into the benefit these innovations can provide to providers and the patients they are treating, including Medicare beneficiaries. RWE is a key component of a value-based health care system and should be incorporated into coverage and payment decisions for programs such as NTAP, pass-through, and other payment programs overseen by CMS.
NPC recommends payment frameworks and public programs consider training, capacity and incentives to ensure that payment and coverage programs build upon the strong foundation provided in the 21st Century Cures Act to enhance the use of RWE.
Patient and Caregiver Voices Should be Incorporated in Coverage Decisions and Payment Incentives
As the United States health care system evolves through the development of new technology and a focus on value-based care, Congress and other stakeholders must continually work to ensure that the voices of patients and caregivers are incorporated. In particular, coverage decisions and policies for payment incentives could greatly benefit from patient and caregiver input.
Coverage decisions should incorporate patient and caregiver feedback
Coverage decisions made by both public and private payors represent a critical area that routinely impacts patients and their caregivers. These decisions have the power to impact a patient’s overall quality of life and encompass important elements of care and cost for the patient, their caregivers, and their providers. One way to accomplish this would be by incorporating the beneficiary perspective into Pharmacy and Therapeutic (P&T) committees or other similar groups. In an era of patient-centered research, consumer-directed health insurance, and other federal and private sector initiatives that actively engage with patients to deliver more appropriate care, the patient or representative beneficiary perspective should be incorporated into the decisions of which treatments to cover.
Outside the United States, health technology assessment (HTA) processes have begun seeking patient and public input to guide resource allocation and coverage decisions.[11,12,13] For instance, the National Institute for Health and Care Excellence (NICE) in the United Kingdom receives input from a panel of 30 members of the public on a range of moral and ethical issues when producing guidance documents. Alternatively, to address questions regarding the patient and caregiver experience, the Scottish Medicines Consortium invites comments from registered patient groups, local support groups, and volunteer organizations after the announcement of a drug appraisal.[14] In the United States, the Department of Defense formulary process presents formulary recommendations to the Beneficiary Advisory Panel, which includes members of the TRICARE beneficiary population, the military’s health plan for active duty and retired uniformed service personnel.[15]
These processes can guide thinking about how to incorporate patient and public input when determining resource allocation and coverage policies. Similar input from patients and consumers to guide beneficiary access to medications in the United States, however, is less common. In a review of standard operating procedures for developing medical policy among 17 of the largest commercial health plans, 15 actively seek specialty provider society or network input. Yet, no health plans offered the same opportunity to seek patient or beneficiary input.[16] The inclusion of patient-beneficiary input in the P&T process can ensure that elements of greatest importance to beneficiaries remain central to health care decision-making and out-of-pocket spending for beneficiaries.
Quality measurement and payment incentives should include patient voices
Another area where the patient voice can be incorporated is payment incentives driven by quality measurement. Patient-focused quality measurement would include patient-reported performance measures (PR-PMs). Patients’ views of quality may differ from those of providers and policymakers, making it vital to include them when designing quality incentive programs. NPC research on quality measurement in value-based performance (VBP) programs found stakeholders have concerns that “value” is often defined from the payer perspective and may not be meaningful to patients and family caregivers.[17] If the measures used in VBP programs are not meaningful to patients, the goal of paying for “value” has not been met.
Including patients in measure and program development is consistent with the principles of national organizations and the strategic goals of CMS:
- NQF identifies patients as the most valuable and authoritative source of information in assessing the quality of health care.[18]
- CMS has a strategic goal to “empower patients and doctors to make decisions about their health care,” and a goal of CMS’ Meaningful Measures framework is to prioritize measures that are meaningful to patients. Including patients and families in OCF program design and measure selection/development can help advance both of these goals at the program level.[19]
- The Blueprint for the CMS Measures Management System also states, “Measure developers should prepare a plan for how patient input will be solicited, gathered and meaningfully incorporated into measure development and maintenance processes…”[20]
The incorporation of PR-PMs is particularly important when individual needs and performances for treatment vary. Few existing PR-PMs address the impact of medications, decision-making or care planning, which are measures that matter to patients. Outcomes that are most important to patients (e.g., symptom control, quality of life) at key points in time (e.g., diagnosis, recurrence, etc.) can encourage stronger patient engagement and aligned incentives.[21] While PR-PMs may differ from condition to condition, where appropriate, cross-cutting PR-PMs should be considered in future policymaking.[22]
For example, research published by NPC and Discern Health in 2019 found that the following strategies would be beneficial for improving patient-reported measures in oncology:
- Involving patients and caregivers throughout all aspects of the measures life cycle to ensure measures capture value;
- Filling care phase and domain gaps in patient-reported measures and PR-PMs;
- Addressing methodological challenges;
- Reducing provider and patient burden by standardizing and aligning the use of both PRMs and PR-PMs; and
- Supporting providers in PRM and PR-PM implementation.[23]
Across many conditions, research has shown that activated patients incur lower health care costs and experience fewer adverse events.
NPC recommends that patients, their caregivers, and other stakeholders are involved throughout all phases of quality measure development, implementation and evaluation. Additional funding to further develop and implement patient-reported measures in quality and value-based programs should be encouraged.
Conclusion
NPC shares Congress’ goal to promote innovation and enhance patient access to life-saving treatments. Thank you for the opportunity to provide comments on Cures 2.0. We hope to continue this important discussion with Congress and other stakeholders.
Sincerely,
Dan Leonard, MA
President and Chief Executive Officer
National Pharmaceutical Council
Jennifer S. Graff, PharmD
Vice President, Comparative Effectiveness Research
National Pharmaceutical Council
-----------
References
[1]MIT NEWDIGS. Precision Financing Solutions for Durable/Potentially Curative Therapies. January 2019. Available at: https://newdigs.mit.edu/sites/default/files/MIT%20FoCUS%20Precision%20Financing%202019F201v023.pdf. Accessed December 13, 2019.
[2] Ibid.
[3] MIT NEWDIGS. Research Brief: State Insurance Regulations Regarding Benefit Design. August 2019. Available at: https://newdigs.mit.edu/sites/default/files/FoCUS%20Research%20Brief_2019F208v040%20Expedited%20Insurance_2.pdf. Accessed December 13, 2019.
[4]Ibid.
[5] Food and Drug Administration (FDA). Framework for FDA’s Real-World Evidence Program. December 2018. Available at: https://www.fda.gov/media/120060/download. Accessed December 13, 2019.
[6] Food and Drug Administration. Submitting Documents Using Real-World Data and Real-World Evidence to FDA for Drugs and Biologics: Guidance for Industry; Draft Guidance. May 2019. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/submitting-documents-using-real-world-data-and-real-world-evidence-fda-drugs-and-biologics-guidance. Accessed December 13, 2019.
[7] Sabharwal RK, Graff JS, Holve E, Dubois RW. Developing Evidence That is Fit for Purpose: A Framework for Payer and Research Dialogue. The American Journal of Managed Care. 2015; 21(9): e545-e551.
[8] Oehrlein EM, Graff JS, Harris J, and Perfetto EM. Patient-Community Perspectives on Real-World Evidence: Enhancing Engagement, Understanding, and Trust. The Patient. 2019; 12(4):375-81.
[9] Chambers JD, Panzer AD, Pope EF, Graff JS, Neumann PJ. Little Consistency in Evidence Cited by Commercial Health Plans for Specialty Drug Coverage. Health Affairs. 2019; 38(11):1882-6.
[10] Malone DC, Brown M, Hurwitz JT, Peters L, Graff JS. Real-World Evidence: Useful in the Real World of US Payer Decision Making? How? When? And What Studies? Value Health. 2018; 21(3):326-33.
[11] Whitty JA. (2013). An International Survey of the Public Engagement Practices of Health Technology Assessment Organizations. Value Health. 2013; 16:155-163.
[12] Rosenber-Yunger ZRS, Bayoumi AM. (2017). Evaluation Criteria of Patient and Public Involvement in Resource Allocation Decisions: A Literature Review and Qualitative Study. International Journal of Technology Assessment in Health Care. 2017; 33(2):270-278.
[13] Facey KM, Hansen HP Single AN (eds). Patient Involvement in Health Technology Assessment. Copyright 2017.
[14] Scottish Medicines Consortium. (2017). Attending a Scottish Medicines Consortium (SMC) meeting: Information for Participating Patient Group Partners. Available at: https://www.scottishmedicines.org.uk/media/2721/information-for-participating-patient-group-partners.pdf. Accessed December 13, 2019.
[15] Lugo AM, Allerman AA, Trice SK. Evolution of the TRICARE Pharmacy Benefit: A Decade of Change. Journal of Managed Care & Specialty Pharmacy. 2019; 25(11):1195-1200.
[16] Caldwell KA, Chambers JD, Graff, JG, Perfetto EM. Patient-Reported Outcomes and Patient Preferences: Considerations for Coverage Policy Decisions? Academy of Managed Care Pharmacy. March 26, 2019. San Diego, CA.
[17] Valuck T, Schmidt T, Perkins B, Patel P, Westrich K, Basch E, McClellan M. Improving patient-reported measures in oncology. February 21, 2019. Available at: https://www.npcnow.org/publication/improving-patient-reported-measures-oncology. Accessed December 2, 2019.
[18] National Quality Forum. Patient-reported outcomes. Available at: https://www.qualityforum.org/Patient-Reported_Outcomes.aspx. Accessed December 2, 2019.
[19] Centers for Medicare and Medicaid Services. Meaningful Measures hub. Available at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/MMF/General-info-Sub-Page. Accessed December 2, 2019.
[20] Centers for Medicare and Medicaid Services. Blueprint for the CMS Measures Management System. Version 15.0. September 2019. Available at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/MMS/Downloads/Blueprint.pdf. Accessed December 2, 2019.
[21] Improving Patient-Reported Measures in Oncology. National Pharmaceutical Council and Discern Health. Available at: https://www.npcnow.org/publication/improving-patient-reported-measures-oncology. Accessed December 6, 2019.
[22] Valuck T, Blaisdell D, Dugan DP, Westrich K, Dubois RW, Miller RS, McClellan M. Improving Oncology Quality Measurement in Accountable Care: Filling Gaps with Cross-Cutting Measures. Journal of Managed Care & Specialty Pharmacy. 2017; 23(2): 174-181.
[23] Improving Patient-Reported Measures in Oncology. National Pharmaceutical Council and Discern Health. Available at: https://www.npcnow.org/publication/improving-patient-reported-measures-oncology. Accessed December 6, 2019.