Patient-Centered Guiding Principles for Evaluating Health Care Spending
NPC established these principles to serve as a checklist to assess whether methods used for estimating health care spending are appropriate.
The first step in addressing health care spending is to accurately diagnose the root causes of increased spending. The diagnosis of root causes requires using transparent, evidence-based and consistently applied methods.
NPC's Patient-Centered Guiding Principles for Evaluating Health Care Spending have two goals:
- Evaluate the rigor and appropriateness of the methods underlying health care spending analyses (i.e., following recommendations from professional associations and other authoritative sources)
- Ensure the alignment of health care spending analyses with patient-centered care
Professional associations and other authoritative sources advance best practices and guidelines for conducting health economic analyses, including health care spending analyses. A few example organizations that have developed standards and best practices relevant for health care spending analyses are the National Health Expenditure Accounts from the Centers for Medicare and Medicaid Services (CMS, 2017), the Triple Aim (expanded to the Quadruple Aim) from the National Academy of Medicine and Consolidated Health Economic Evaluation Reporting Standards (CHEER) from ISPOR--The Professional Society for Health Economics and Outcomes Research.
For these principles, we define “health care spending analyses” as analyses of health care spending above the individual service or treatment level. Examples of health care spending analyses include segment-level (e.g., inpatient, drug, office), condition-specific aggregate spending, population-level, and organization-level (e.g., accountable care organizations, hospitals) analyses.
Each guiding principle includes four components: (1) a definition, (2) supporting detail and citation(s) to provide additional context and clarity, (3) a brief description of how to use the principle and (4) an illustrative example.
Evaluation of Health Care Spending Should:
1.1 Consider impacts of changes in health spending on patients and society (Institute of Medicine, 2011)
Supporting Detail
Health care spending analyses should be grounded in patient-centered care, which the Institute of Medicine defines as “Providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions” (Institute of Medicine, 2011). As such, policy recommendations should consider the tradeoffs between health care spending changes and their potential impacts on outcomes important to patients and society. Examples of outcomes to consider include patient health and functioning, patient experience, patient financial burden, patient access to care, caregiver burden and productivity.
How to Use This Guiding Principle
When assessing the consistency of a health care spending analysis with patient-centered care, the reviewer should confirm that the analysis accounts for the effects on outcomes important to patients and society. When data on outcomes that are most important to patients and society are not available, the discussion should note this critical limitation and whether deference was given to patients’ needs.
Illustrative Example
In a study of expenditure data from health departments in Florida and Washington, Bekemeier and colleagues examined the potential influence of states’ investment in maternal and child health services on population health outcomes (Bekemeier et al., 2014). They estimated the relationship between the level of investment in various services and critical indicators of family health in the population (i.e., the prevalence of low birth weight and infant mortality). Investments included expenditures for the Women, Infants, and Children Program, family planning, and maternal, infant, child and adolescent
health. The authors concluded that there are long-term health benefits from investments in public maternal and infant care services, especially in populations living in poverty.
The following (Assessment 1) summarizes how this study assessed policy performance based on impacts to patients and society.
Assessment 1. Evaluation of the Bekemeier Study (Bekemeier et al., 2014)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the analysis account for the impacts of differences in health spending on the population outcomes important to patients and society? | The study assessed the impact of maternal and child health services spending on the prevalence of low birth weight and infant mortality. The authors explained that low birth weight contributes to a significant burden to society, including high direct medical costs, higher childcare expenses and increased caregiving burden. |
| 2 | If applicable, did the study acknowledge the limitation and implications of excluding key outcomes? Was deference given to patients’ needs? | Not applicable. |
1.2 Incorporate estimates of the actual amounts paid for medical care (White and Whaley, 2019; IQVIA Institute for Human Data Science, 2021)
Supporting Detail
There are significant variations between U.S. list prices/charged amounts and actual/net amounts paid for medical care (White and Whaley, 2019; IQVIA Institute for Human Data Science, 2021). Therefore, health care spending analyses should incorporate estimates of actual/net amounts paid by relevant parties (i.e., the patient, the health care provider and the third-party payer). If actual/net amounts paid are unavailable, sensitivity analysis should examine potential variations between charged amounts/list prices and actual paid amounts.
How to Use This Guiding Principle
The reviewer should confirm that spending estimates use actual/net paid amounts for each relevant stakeholder (i.e., payers, patients, providers). When actual/net paid amounts are not available, the study should incorporate appropriate estimates and provide clear documentation on how the estimates of amounts paid were calculated. In general, the actual/net amounts paid for medical care services and prescription medications vary significantly within stakeholder type. The amount paid is often unavailable to researchers. In this case, the study should document assumptions used to estimate amounts paid and test these assumptions in comprehensive sensitivity analyses.
Illustrative Example
Hernandez and colleagues studied the difference between the list and net prices of branded pharmaceutical products between 2007 and 2018, using a database that included rebate estimates (Hernandez et al., 2020). The study found that list prices increased by almost 160% (9.0% average per year), but net prices increased by only 60% (4.4% average per year) (see Table 2). Due to significant differences in the list and net price, the authors concluded that the use of list prices would
overestimate payers’ drug costs.

The following (Assessment 2) assesses the use of actual paid amounts in this health care spending analysis.
Assessment 2. Evaluation of the Hernandez Study (Hernandez et al., 2020)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Was the spending calculated using estimates of the actual/net amounts paid by stakeholders relevant to the analysis for the sources of medical care under evaluation? | The study evaluated the U.S. payers’ perspective; therefore, it considered drug prices paid by payers by type (i.e., Medicaid vs. non-Medicaid). |
| 2 | Did the study document the estimation of actual/net paid amounts for each relevant stakeholder? | The study used estimated net prices. Net price is product unit revenue less manufacturer concessions (rebates, coupon cards, discounts, return provisions and other deductions accounted for in the reporting of sales). |
| 3 | If the amount paid was unavailable to the author, did the study document assumptions used to estimate amounts paid and test these assumptions in comprehensive sensitivity analyses? | The study reported multiple limitations. For example, net pricing data is limited to branded products owned by publicly traded companies. |
1.3 Recognize differences in spending across patients and time (Dieleman et al., 2017)
Supporting Detail
Rather than focusing solely on mean or median changes in health care spending for patients with a specific condition, health care spending analyses should consider the distribution of per-patient costs resulting from differences in patients’ ages, underlying health conditions, comorbidities, and severity and treatment/utilization patterns resulting from changes in clinical practice or patient access [e.g., coverage policy, benefit design (including out-of-pocket responsibility)]. This distribution should be examined across both patients and time. Doing so can provide a more comprehensive assessment of health care spending and help identify the variance in and root causes of health care spending for specific health conditions (Dieleman et al., 2017). It may not be possible to perform this type of analysis when dealing with small patient populations such as those with a rare disease.
How to Use This Guiding Principle
Health care spending analyses should report results for both the total population and critical subpopulations that may differ from the population average. Further, studies analyzing changes over time should incorporate corresponding changes in the demographics, treatment and utilization patterns (resulting from changes in clinical practice or patient access, including financial burden), and key population health outcomes. Therefore, studies should always report their rationale for selecting specific analyses to account for differences in health care spending across patients and time. Researchers may not always have access to data to conduct rigorous subpopulation analyses or time-series assessments of changes in underlying population health and treatment or utilization patterns. In addition, the patient population may be too small to conduct this type of analysis, especially for rare diseases. In these circumstances, researchers should document the lack of data as a limitation of the study.
Illustrative Example
In a study of patients with heart failure (Yoon et al., 2016), the authors reported the average per-patient cost of heart failure and factors that may contribute to higher costs. The annual cost of heart failure depended on the patient’s age, race or ethnicity, history of substance abuse and comorbid conditions.
The following (Assessment 3) summarizes methods that this study used to account for differences in spending across patients and time.
Assessment 3. Evaluation of the Yoon Study (Yoon et al., 2016)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | The authors reported demographic and clinical risk factors for high spending. | The authors reported demographic and clinical risk factors for high spending. |
| 2 | If the study analyzed changes over time, did it report changes in the demographics, treatment/ utilization patterns, patient access and key population health outcomes during the studied time frame? If not, was the rationale for not including them documented? | Not applicable because the study did not compare health care spending over time. |
1.4 Account for changes in disease- or condition-specific epidemiologic measures such as incidence and prevalence (Dieleman et al., 2017)
Supporting Detail
Changes in condition-specific epidemiologic measures contribute to health care spending changes (Dieleman et al., 2017). For example, disease-specific spending could increase with time due to prevalence increases while individual treatment costs decline. Focusing solely on disease-specific spending would miss the fact that treatment costs per patient are declining. Therefore, health care spending for diseases and conditions should be estimated in two ways: (1) for all people living with
the condition and (2) for an individual living with the condition. This approach eliminates confounding from changes in the number of new cases each year or changes in the number of people living with a chronic condition because of behavioral, environmental, prophylactic therapy, treatment or public health changes.
How to Use This Guiding Principle
Health care spending analyses should report both population-level and patient-level spending. Suppose the study reports overall health care spending only. In that case, authors should document this limitation and state the implications of omitting the estimates adjusted by the disease prevalence.
Illustrative Example
In comparing U.S. and western European countries, Thorpe and colleagues examined how disease prevalence and treatment rates may have affected the per-capita health care spending for the 10 most costly conditions in the U.S. and European countries (Thorpe et al., 2007). Based on an analysis of data from surveys of the noninstitutionalized population aged 50 years and older, this study found the prevalence and rates of medication treatment for almost all of the 10 conditions examined were considerably higher in the U.S. than in European countries. The authors concluded that these findings indicate the importance of health policies aligned with goals to reduce the prevalence of chronic illness.
The following (Assessment 4) summarizes methods that this study used to account for changes in disease- or condition-specific epidemiologic measures.
Assessment 4. Evaluation of the Thorpe Study (Thorpe et al., 2007)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the study report health care spending both at the per-person and population levels? |
After reporting differences in disease prevalence and treatment rate as potential factors for the higher per-capita health care spending in the U.S. vs. Europe, this study did not report health care spending per person for each condition. The authors reported that estimating the cost per diagnosed case of each condition would have been challenging. |
1.5 Be adjusted for inflation (Dunn et al., 2018)
Supporting Detail
Analyses should incorporate inflation to adjust rising health care spending for base changes in costs of goods and labor (Dunn et al., 2018). Examples of appropriate indexes include the Consumer Price Index for All Urban Consumers and the gross domestic product (GDP) implicit price deflator.
How to Use This Guiding Principle
Health care spending analyses should report the year of the data used to estimate spending and indicate which index was used to adjust for general inflation. The reviewer should evaluate whether the index was appropriate in the context of the analysis. If not adjusted for inflation, the reviewer should (1) confirm whether the study provides a rationale for the approach and (2) evaluate the implication of using unadjusted health care spending.
The analysis context will determine the most appropriate inflation index (Dunn et al., 2018). For example, an analysis from the societal perspective should use the GDP implicit price deflator. In contrast, analysis from the patient perspective should consider the overall Personal Consumption Expenditures (PCE) index to adjust health expenditures in terms of purchasing power. Either the Personal Health Care deflator or the PCE health-by-function index can be used to adjust spending associated with a specific disease. However, the Producer Price Index should be used to adjust inpatient service expenditures.
Illustrative Examples
In a study of changes in spending for 155 health conditions between 1996 and 2013, the authors adjusted all components of health spending estimates into 2015 dollars to account for inflation. In addition, the spending estimates were actual amounts paid (vs. charges) (Dieleman et al., 2017). The authors adjusted costs using the economy-wide consumer price index from the International Monetary Fund.
The following (Assessment 5) summarizes methods this study used to account for inflation.
Assessment 5. Evaluation of the Dieleman Study (Dieleman et al., 2017)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the study report the year of the data used to estimate the spending? | The study reported various data sources used to estimate health spending and the years of the data for each source. |
| 2 |
Did the study adjust spending data for general inflation?
|
The study adjusted all spending data to be expressed in 2015 dollars and used an appropriate index. |
1.6 Be based on data relevant to the analysis objectives (Smith et al., 2018)
Supporting Detail
It is critical to ensure that data selected are relevant to the specific objectives of the spending analysis, the relevant population and the relevant observational period (Smith et al., 2018). The research should provide precise descriptions of the studied population, analysis metrics and data collection period. Furthermore, the study should discuss the generalizability of its findings. For example, suppose study data underrepresent certain populations (e.g., the uninsured population, the unemployed). In that case, the study should state who is included and excluded from spending estimates and how using such data may impact the interpretation of the study results.
How to Use This Guiding Principle
When evaluating a health care spending analysis, the reviewer should confirm that the analysis is accompanied by clear descriptions of the population studied and the period of analysis. In addition, the study should discuss the generalizability of its outcomes.
Illustrative Example
Cutler and colleagues (2019) examined reasons for the slowdown in per-capita spending for Medicare beneficiaries between 1999 and 2012 based on an analysis of the Medicare Current Beneficiary Survey (MCBS) (Cutler et al., 2019). To address the exclusion of Medicare Advantage enrollees’ claims from the study data, the study reweighted data so that the population represented in the data matched the socioeconomic and health statuses of the total Medicare beneficiaries, including Medicare Advantage recipients. The study then validated the weighting method by ensuring that the estimated service-specific spending matched national totals in another database, the National Health Expenditure Accounts.
The following (Assessment 6) summarizes how this study ensured the data used for the analysis were relevant to the analysis objectives.
Assessment 6. Evaluation of the Cutler Study (Cutler et al., 2019)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the study provide precise descriptions of its metrics, the population studied and the study period? | To estimate the aggregate spending among Medicare beneficiaries between 1999 and 2012, the authors used a database of Medicare beneficiaries, MCBS (1999-2012). |
| 2 | Did the study discuss the generalizability of its findings? | Because MCBS did not include Medicare Advantage enrollee claims, the study implemented a weighting method to correct the potential bias from this limitation. Further, the study concluded that the implications of the future of cost growth are unclear due to various environmental factors that are difficult to predict. |
1.7 Be accompanied by sensitivity analyses to elucidate uncertainty that may exist in the evaluation (Walker and Fox-Rushby, 2001)
Supporting Detail
Health care spending analyses should acknowledge the inherent uncertainty associated with health care spending data (Walker and Fox-Rushby, 2001). Specifically, the study should vary unit cost and utilization pattern assumptions when actual values range or are assumed. Unit cost-related assumptions include reimbursement rates, discounts/rebates, patient cost share and payer mix.
Utilization-related variables include patient mix characteristics, coverage, payer mix and treatment patterns. The purpose of varying unit costs and utilization-related variables is to determine whether the study’s conclusions are valid across a range of reasonable assumptions.
How to Use This Guiding Principle
Rigorous sensitivity analyses should accompany health care spending analyses. Specifically, the researcher should test the impact of critical assumptions by demonstrating how changing these assumptions affect the overall study results. The study also should address the potential effects of uncertainty by (1) reporting confidence intervals, standard deviations or standard errors around each key analysis input and (2) demonstrating the effects of parameter uncertainty by varying key input values on analysis results.
Illustrative Example
Irwin and colleagues analyzed the impact of a supervised injection facility on opioid-dependent individuals in Baltimore. Specifically, the study reviewed population-level outcomes and reduced health care spending resulting from lower resource use (Irwin et al., 2017). Population-level outcomes reported were the number of human immunodeficiency virus (HIV) and hepatitis C transmissions prevented, skin infections prevented and overdose deaths prevented. For health care resource metrics, the study reported overdose-related medical care and medication-assisted treatments. The researchers conducted sensitivity analyses by varying each of the critical model inputs to estimate the range of net savings after instituting a supervised injection facility.
The following (Assessment 7) summarizes how this study accounted for uncertainty around data used for the analysis.
Assessment 7. Evaluation of the Irwin Study (Irwin et al., 2017)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the study examine how changing critical assumptions affected the overall study results? | Key assumptions such as the facility operating cost, syringe-sharing rate, soft-tissue infection rate, overdose rate, overdose death rate and referral rate for medication-assisted treatment were varied by ±50%. |
| 2 | Did the study report confidence intervals, standard deviations or standard errors around each key analysis input? | The study did not report descriptive statistics around any of the model inputs used to estimate outcomes. |
| 3 | If the analysis used an economic model, did the study conduct sensitivity analyses around inputs’ parameter uncertainty? | The study did not conduct any sensitivity analysis informed by statistical inference; all sensitivity analyses used arbitrary ranges. |
1.8 Place conclusions and policy recommendations in the appropriate context (Husereau et al., 2013)
Supporting Detail
Findings and conclusions of spending analyses require appropriate context (Husereau et al., 2013). When applicable, study findings and recommendations should incorporate (1) how the findings or policy recommendations may impact all relevant stakeholders (e.g., patients, caregivers and society); (2) the costs, outcomes, and cost relative to the benefits that are important to the relevant stakeholders; (3) how the study’s findings are supported by its results; (4) the study’s limitations and uncertainty; and (5) the potential tradeoffs between cost savings and the delivery of care, the impact on downstream population health, and other relevant outcomes.
How to Use This Guiding Principle
Conclusions and policy recommendations in the appropriate context will satisfy the following requirements: (1) The study analyzes and clearly states the impact of changes for all relevant stakeholders; (2) the impact analysis includes the costs, outcomes, and cost relative to the benefit measures that are important to the relevant stakeholders; (3) the study’s results justify the conclusions and policy recommendations; (4) the conclusions and policy recommendations appropriately consider the study’s limitations and uncertainty; and (5) the study clearly states both short- and long-term potential tradeoffs between cost savings and impacts. The study should consider impacts on the delivery of care, downstream population health and other relevant patient outcomes.
Illustrative Example
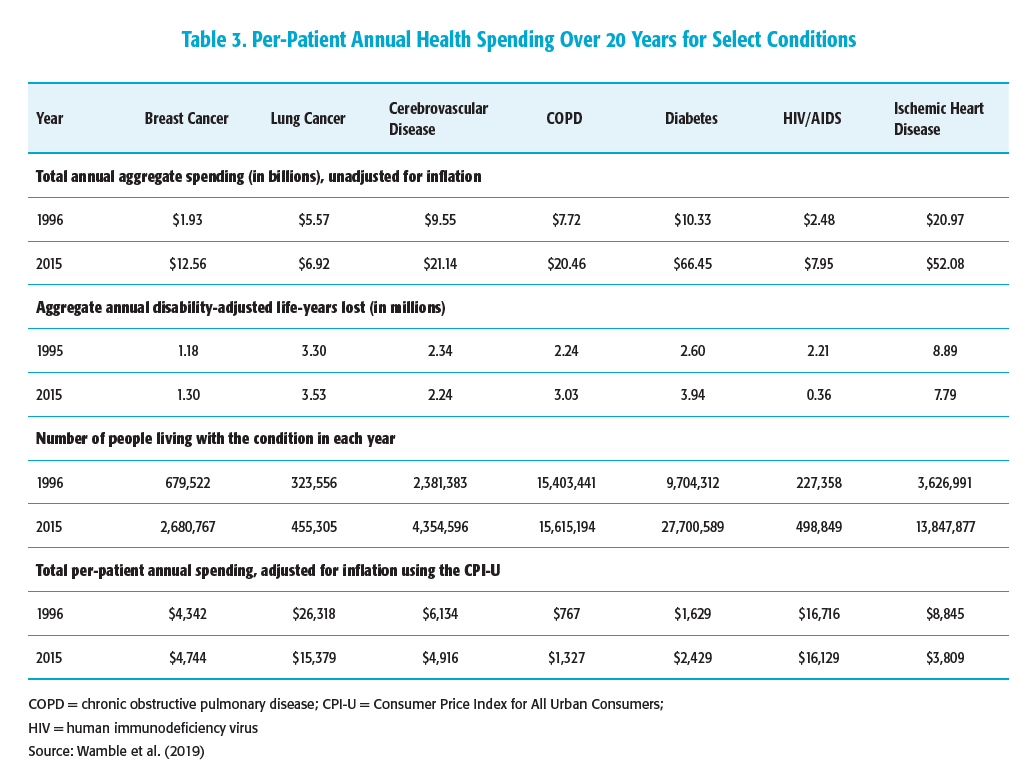
In a study based on the Medical Expenditure Panel Survey and Global Burden of Disease databases, Wamble and colleagues assessed changes in aggregate annual health care spending across conditions with high mortality and morbidity rates between 1996 and 2015 (Wamble et al., 2019). To better understand the outcomes associated with changes in aggregate health care spending across conditions evaluated, the authors estimated the changes in aggregate annual disability-adjusted life-years (DALYs) lost for each condition and the prevalence of each condition during this period. As presented in Table 3, some of the increase in aggregate spending may be explained by the increased prevalence of the condition, the improved outcomes and inflation between 1996 and 2015. For instance, although the total spending for HIV/AIDS more than tripled between 1996 and 2015 when unadjusted for inflation, per-person annual spending adjusted for inflation using the Consumer Price Index for All Urban Consumers actually decreased, because the number of people living with HIV/AIDS more than doubled. Furthermore, the DALYs lost were reduced by more than sixfold because of the availability of improved treatment regimens that lowered death rates and decreased morbidity.
The following (Assessment 8) summarizes whether the above study placed conclusions and policy recommendations in the appropriate context.
Assessment 8. Evaluation of the Wamble Study (Wamble et al., 2019)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the study analyze and clearly state the impact of changes for all relevant stakeholders? | The study analyzed the relationship between health care spending increases and improvements in health. Results were for the entire U.S. population (vs. reporting separate estimates of spending for patients, public payers and private payers). The analysis did not include subpopulations. |
| 2 | Did the impact analysis include the costs, outcomes, and cost relative to the benefit measures that are important to the relevant stakeholders? | The study considered both costs and benefits. The analysis used annual changes in total costs of care per patient as the cost measure. In parallel, yearly changes in DALYs per patient were the mortality and morbidity measure. The study did not include direct costs (e.g., OOP) to the patient. |
| 3 | Did the study’s results justify the conclusions and policy recommendations? | The study had three policy implications: First, focusing on cost alone may lead to bad policies. This conclusion is justified, since the data show that increasing costs can be a source of value. Second, the study states that increased costs can be a source of high value in some conditions. The study found that increased costs were a source of high value for several of the diseases analyzed. The third conclusion is that the value of cost increases varies; therefore, policies should protect high-value creation and reduce low-value creation at the disease level. The varying results by disease support the need for this type of approach, but the authors do not consider implementation barriers to this approach. |
| 4 | Did the conclusions and policy recommendations appropriately consider the study’s limitations and uncertainty? | The authors noted that the critical limitation of the study was that the base-case analysis assumed all improvements in population health outcomes were due to medical interventions. The authors recognized that the improved health outcomes could be attributable to public health factors and improved medical treatment. The authors explored the impacts of different allocations of health improvements between public health changes and medical care improvement. The sensitivity analysis did not alter the study conclusions. The authors also discussed several database specific limitations, which may affect the generalizability of the results. |
| 5 | Did the study clearly state both short- and long-term potential tradeoffs between cost savings and impacts? Did the study consider effects on the delivery of care, downstream population health and other relevant patient outcomes? | The policy implications considered the tradeoffs between cost containment and population health. The study did not consider the potential tradeoffs of using cost savings for other high-value investments. Impacts on the delivery of care were not applicable here. |
References
Adler NE, Prather AA. 2015. “Determinants of Health and Longevity.” Population Health: Behavioral and Social Science Insights. Rockville, MD: Agency for Health Care Research and Quality. Available at http://www.ahrq.gov/professionals/education/curriculum-tools/population-health/adler.html. Accessed July 7, 2020.
American College of Physicians. 2009. “Controlling Health Care Costs While Promoting the Best Possible Health Outcomes.” Available at https://www.acponline.org/acp_policy/policies/controlling_healthcare_costs_2009.pdf. Accessed August 3, 2020.
American College of Physicians. 2021. “What Is the Patient-Centered Medical Home?” Available at https://www.acponline.org/practice-resources/business-resources/payment/delivery-and-payment-models/patient-centered-medical-home/understanding-the-patient-centered-medical-home/what-is-the-patient-centered-medical-home. Accessed March 23, 2021.
Artiga S, Hinton E. 2018 (May 10). “Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity.” Available at https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/. Accessed August 3, 2020.
Baicker K. 2019. “Economic Analysis for Evidence-Based Health Policy: Progress and Pitfalls.” Natl Bureau Econ Res Report. 3:1-6.
Bisognano M, Kenney C. 2012. Pursuing the Triple Aim: Seven Innovators Show the Way to Better Care, Better Health, and Lower Costs. New York: John Wiley & Sons.
Bekemeier B, Yang Y, Dunbar MD, Pantazis A, Grembowski DE. 2014 (June). “Targeted Health Department Expenditures Benefit Birth Outcomes at the County Level.” Am J Prev Med. 46(6):569-77.
Blume-Kohout M, Sood N. 2013. “Market Size and Innovation: Effect of Medicare Part D on Pharmaceutical Research and Development.” J Public Econ. 97:327-36.
Cantor J, Torres A, Abrams C, Elbel B. 2015 (November). “Five Years Later: Awareness of New York City’s Calorie Labels Declined, with No Changes in Calories Purchased.” Health Aff (Millwood). 34(11):1893-900.
Centers for Disease Control and Prevention (CDC). 2010 (October). “Establishing a Holistic Framework to Reduce Inequities in HIV, Viral Hepatitis, STDs, and Tuberculosis in the United States.” Atlanta (GA): U.S. Department of Health and Human Services, CDC.
Centers for Medicare and Medicaid Services (CMS). 2017. “National Health Expenditure Accounts: Methodology Paper.” Available at https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/dsm-17.pdf. Accessed July 6, 2020.
Crits-Christoph P, Gallop R, Noll E, et al. 2018 (August). “Impact of a Medical Home Model on Costs and Utilization among Comorbid HIV-Positive Medicaid Patients.” Am J Manag Care. 24(8):368-75.
Cutler DM, Ghosh K, Messer KL, Raghunathan TE, Stewart ST, Rosen AB. 2019 (February). “Explaining the Slowdown in Medical Spending Growth Among the Elderly, 1999-2012.” Health Aff (Millwood). 38(2):222-9.
Cylus J, Papanicolas I, Smith PC. 2016. “A Framework for Thinking about Health System Efficiency.” Available at https://www.ncbi.nlm.nih.gov/books/NBK436891/. Accessed February 18, 2021.
Dieleman JL, Squires E, Bui AL, et al. 2017. “Factors Associated With Increases in U.S. Health Care Spending, 1996-2013.” JAMA. 318:1668-78.Dorn S. 2019 (June 18) “The Cadillac Tax: It’s Time To Kill This Policy Zombie.” Health Affairs blog. Available at https://www.healthaffairs.org/do/10.1377/hblog20190617.795057/full/.
Dunn A, Grosse SD, Zuvekas SH. 2018 (February). “Adjusting Health Expenditures for Inflation: A Review of Measures for Health Services Research in the United States.” Health Serv Res. 53(1):175-96.
Elbel B, Kersh R, Brescoll VL, Dixon LB. 2009 (November-December). “Calorie Labeling and Food Choices: A First Look at the Effects on Low-Income People in New York City.” Health Aff (Millwood). 28(6):w1110-21.
Hardin L, Kilian A, Murphy E. 2017. “Bundled Payments for Care Improvement Preparing for the Medical Diagnosis-Related Groups.” J Nurs Admin. 47(6):313-9.
Husereau D, Drummond M, Petrou S, et al. 2013. “Consolidated health economic evaluation reporting standards (CHEERS)—explanation and elaboration: a report of the ISPOR health economic evaluation publication guidelines good reporting practices task force.” Value in Health. 16.2: 231-250.
Hernandez I, San-Juan-Rodriguez A, Good CB, Gellad WF. 2020 (March 3) “Changes in List Prices, Net Prices, and Discounts for Branded Drugs in the U.S., 2007-2018.” JAMA. 323(9):854-62.
Institute of Medicine. 2010. “The Healthcare Imperative: Lowering Costs and Improving Outcomes: Workshop Series Summary.” Washington, DC: The National Academies Press. Available at https://doi.org/10.17226/12750.
Institute of Medicine. 2011. “Patients Charting the Course: Citizen Engagement and the Learning Health System: Workshop Summary.” Washington, DC: The National Academies Prehttps://doi.org/10.17226/13444ss. Available at https://doi.org/10.17226/12848. Accessed July 23, 2021.
Institute of Medicine. 2013. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Washington, DC: The National Academies Press. Available at https://doi.org/10.17226/13444.
IQVIA Institute for Human Data Science. 2021 (May). “The Use of Medicines in the U.S.: Spending and Usage Trends and Outlook to 2025.” Available at https://www.iqvia.com/insights/the-iqvia-institute/reports/the-use-of-medicines-in-the-us. Accessed June 28, 2021.
Irwin A, Jozaghi E, Weir VW, Allen ST, Lindsay A, Sherman SG. 2017 (May 12). “Mitigating the Heroin Crisis in Baltimore, MD, USA: A Cost-Benefit Analysis of a Hypothetical Supervised Injection Facility.” Harm Reduct J.14(1):29.
Landers RM, Vladeck B, Cole BK. 2020 (March 23). “Medicare’s Current and Future Role in Reducing Racial and Ethnic Health Disparities.” Health Affairs blog. Available at https://www.healthaffairs.org/do/10.1377/hblog20200319.932279/full/. Accessed March 22, 2021.
LaPointe J. 2020. “CMS Releases Initial Report on Risk-Based Bundled Payment Model.” Available at https://revcycleintelligence.com/news/cms-releases-initial-report-on-risk-based-bundled-payment-model. Accessed July 7, 2020.
McClellan MB, Feinberg DT, Bach PB, et al. 2017 (March 17). “Payment Reform for Better Value and Medical Innovation.” NAM Perspectives. Available at https://nam.edu/wp-content/uploads/2017/03/Payment-Reform-for-Better-Value-and-Medical-Innovation.pdf. Accessed February 22, 2021.
National Quality Forum. 2009. “Measurement Framework: Evaluating Efficiency Across Patient-Focused Episodes of Care [abstract].” Available at https://www.qualityforum.org/Publications/2010/01/Measurement_Framework__Evaluating_Efficiency_Across_Patient-Focused_Episodes_of_Care.aspx. Accessed July 7, 2020.
Peter G. Peterson Foundation. 2020 (April 20). “Why Are Americans Paying More for Health Care?” Available at https://www.pgpf.org/blog/2020/04/why-are-americans-paying-more-for-health care. Accessed August 3, 2020.
Revere L, Kavertapu N, Hall J, Begley C. 2020. “Achieving Triple Aim Outcomes: An Evaluation of the Texas Medicaid Waiver.” Inquiry. 57:0046958020923547.
Richardson H, Budros M, Chernew ME, Fendrick AM. 2019 (July 15). “V-BID X: Creating a Value-Based Insurance Design Plan for the Exchange Market.” Health Affairs blog. Available at https://www.healthaffairs.org/do/10.1377/hblog20190714.437267/full/. Accessed March 22, 2021.
Smith M, Lix LM, Azimaee M, Enns JE, Orr J, Hong S and Roos LL. 2018 (March 1). “Assessing the Quality of Administrative Data for Research: A Framework from the Manitoba Centre for Health Policy.” J Am Med Inform Assoc. 25(3):224-29.
The National Health Council. 2019 (June). “The National Health Council Rubric to Capture the Patient Voice: A Guide to Incorporating the Patient Voice into the Health Ecosystem.” Available at https://www.nationalhealthcouncil.org/Patient-Engagement-Rubric. Accessed August 4, 2020.
The Lewin Group. 2021 (March). “CMS Bundled Payments for Care Improvement Initiative Models 24: Year 7 Evaluation & Monitoring Annual Report.” Available at https://innovation.cms.gov/data-and-reports/2021/bpci-models2-4-yr7evalrpt. Accessed May 10, 2021.
Thorpe KE, Howard DH, Galactionova K. 2007 (November-December). “Differences in Disease Prevalence as a Source of the U.S.-European Health Care Spending Gap.” Health Aff (Millwood). 26(6):w678-86.
Tran LD, Zimmerman FJ, Fielding JE. 2017. “Public Health and the Economy Could Be Served by Reallocating Medical Expenditures to Social Programs.” SSM Popul Health. 3:185-91.
VBID Health. 2017. “Tackling the epidemic of low-value spending and medical overuse: opportunities for purchasers and carriers.” Available at http://www.vbidhealth.com/docs/TF-LVC-%20White%20Paper%20-%20October%20Draft.pdf. Accessed August 3, 2020.
Walker D, Fox-Rushby J. 2001 (December). “Allowing for Uncertainty in Economic Evaluations: Qualitative Sensitivity Analysis.” Health Policy Plan. 16(4):435-43.
Wamble D, Ciarametaro M, Houghton K, Ajmera M, Dubois RW. 2019 (January). “What’s Been the Bang for the Buck? Cost-Effectiveness of Health Care Spending Across Selected Conditions in the U.S.” Health Aff (Millwood). 1;38(1):68-75.
Washington Health Initiative. 2019 (October). “Right Care: First, Do No Harm: Calculating Health Care Waste in Washington State Multi-Year and Medical Group Results.” Available at https://www.wacommunitycheckup.org/media/47217/first-do-no-harm-oct-2019.pdf. Accessed June 10, 2021.
Warshawsky MJ, Leahy M. 2018 (April). “Affordable Care Act’s Cadillac Tax Could Affect One-Fourth of Workers With Employer Health Coverage by 2025.” Health Aff (Millwood). 37(4):613-18.
White C, Whaley CM. 2019. “Prices Paid to Hospitals by Private Health Plans Are High Relative to Medicare and Vary Widely: Findings From an Employer-Led Transparency Initiative.” Available at https://www.rand.org/pubs/research_reports/RR3033.html. Accessed August 3, 2020.
Wyatt R, Laderman M, Botwinick L, Mate K, Whittington J. 2016. “Achieving Health Equity: A Guide for Health Care Organizations.” Institute for Health Care Improvement. Available at http://www.ihi.org/resources/Pages/IHIWhitePapers/Achieving-Health-Equity.aspx. Accessed February 22, 2021.
Yoon J, Fonarow GC, Groeneveld PW, Teerlink JR, Whooley MA, Sahay A, Heidenreich PA. 2016. “Patient and Facility Variation in Costs of V.A. Heart Failure Patients.” JACC Heart Fail. 4(7):551-8.
These Patient-Centered Guiding Principles for Evaluating Health Care Spending are one part of NPC's Health Care Spending Guiding Principles. Click here for the Patient-Centered Guiding Principles for Reforming Health Care to Address Rising Health Care Spending.
Read the Full Health Care Spending Guiding Principles
These principles are intended to guide a rigorous, evidence-based evaluation and discussion of health care spending estimates and policies. They aim to improve health care spending efficiency and maximize patient health.