Patient-Centered Guiding Principles for Reforming Health Care to Address Rising Health Care Spending
NPC established these principles to assess health care spending policies to ensure alignment with the goals of patient-centered care.

Policies to curb rising U.S. health care spending must be grounded in rigorous research. They should aim to control costs and promote high-value care without unintended consequences that could negatively affect patient health.
NPC's Patient-Centered Guiding Principles for Reforming Health Care to Address Rising Health Care Spending have two goals:
- Establish patient-centered principles to guide reforms addressing rising health care spending
- Provide a set of standards to evaluate individual health policies against the goals of patient-centered care
These principles can be used to evaluate legislative, regulatory, and payer policies to reform health spending. For these principles, health care spending policy is defined as health system or health plan policies that attempt to control or redistribute health care spending at a level above the individual service or treatment level. Examples of health care spending policy include, but are not limited to, changes in reimbursement approaches (e.g., alternative payment approaches, greater use of budget caps), benefit design (e.g., greater use of high deductible health plans, tax deductions for health insurance premiums), and coverage policies (e.g., exclusion of low-value care services, narrow networks of providers), as well as structural changes to the health system (e.g., elimination of drug rebates, price capitation).
Each guiding principle includes four components: (1) a definition, (2) supporting detail and citation(s) to provide additional context and clarity, (3) a brief description of how to use the principle and (4) an illustrative example. While these principles are intended to evaluate health care policy reforms prospectively, the examples included here are retrospective for illustration.
Policies Reforming Health Care Spending to Address Rising Spending Should:
2.1 Be designed to achieve the intention of the Triple Aim framework of health care improvement (Bisognano et al., 2012)
Supporting Detail
As stated in the Triple Aim framework developed by the Institute for Healthcare Improvement (IHI), “in order to optimize the performance of the U.S. health care system, a policy needs to be designed to pursue the following aims simultaneously: (1) improving the patient experience of care (including quality and satisfaction), (2) improving the health of populations and (3) reducing per-capita costs of health care” (Bisognano et al., 2012). Overall reform efforts should focus on all three prongs of the Triple Aim framework, while the goals of individual policies may focus on a subset. However, reduced per-capita costs should not be achieved at the expense of the patient experience or population health.
Furthermore, the goal of reducing per-capita costs of health care should not prevent the adoption of high-value care that increases costs. Furthermore, the IHI stated that “the Triple Aim will not be achieved until it is achieved for all” (Wyatt et al., 2016). Thus, policymakers should design health care spending policies that achieve all three aims for all people. Specifically, these policies should improve quality of care and health outcomes for those groups of individuals historically linked to discrimination or exclusion such as racial and ethnic minorities, religious minorities, populations based on gender and sexual orientation, people with mental and physical disabilities, and the socioeconomically disadvantaged.
How to Use This Guiding Principle
The goal of any policy reform framework and every specific policy to moderate health care spending should be consistent with that of the Triple Aim framework. Reviewers should assess the following three potential policy impacts: (1) patient experience of care, (2) population health and (3) per-capita costs. Policies should not advance cost reductions at the expense of patient experience of care and population health. In addition, per guiding principle 2.7, health spending policies should not prevent the adoption of high-value patient care that increases costs.
Illustrative Example
The Delivery System Reform Incentive Payment (DSRIP) program in Texas is a Medicaid waiver program that began in 2011. Underpinning the DSRIP are the Triple Aim framework goals of improving population health, enhancing the patient care experience and reducing costs within the Medicaid and low-income uninsured (MLIU) population in Texas. Under the first waiver, DSRIP 1.0 (2011-2017), the participating providers, led by a regional coordinator, carried out a regional health care needs assessment focused on unmet needs within the MLIU population. Based on the review, providers selected from the state menu of infrastructure and service redesign projects that addressed one or more regional needs. Providers were paid to design and implement innovative projects and achieve health outcome improvements in patients served by these projects.
The second waiver, DSRIP 2.0, which began in October 2017, maintained the regional health care partnerships structure. However, it required providers to define their populations at the broader system level (e.g., all patients served by the major components of a provider’s health system vs. patients served by specific projects).
Revere and colleagues conducted an evaluation of DSRIP 1.0 and 2.0 by mapping the significant features of the program and the Triple Aim framework objectives.
The Revere study noted that there was a substantial increase, at a general level, in the effectiveness of care and patient-centered care metrics under DSRIP 1.0. Although there were continued increases seen in performance metrics under DSRIP 2.0, the change to a broader system-level focus under DSRIP 2.0 and the resultant expansion of the MLIU study population resulted in a flattening in the trajectory of improvement when compared to the metrics seen in DSRIP 1.0.
Contrarily, some metrics worsened over the one-year DSRIP 2.0 measurement period. For example, the latent tuberculosis infection treatment rate declined by 27%, and controlling for high blood pressure decreased by 7%. Furthermore, when using utilization as a proxy for costs, it was unclear whether DSRIP reduced costs. Between the baseline year and performance year three in DSRIP 1.0, the authors observed a reduction in 30-day hospital re-admissions for most causes and emergency department (ED) visits for behavioral health and substance abuse. However, the other utilization measures, including mental health admissions and re-admissions and ED visits for diabetes, showed increased utilization. In DSRIP 2.0, only two measures (risk-adjusted congestive heart failure 30-day re-admissions and risk-adjusted all-cause re-admissions) showed improved utilization. The remaining utilization metrics (i.e., ED visits for behavioral health and substance abuse, behavioral health and/or substance abuse 30-day re-admissions, mental health admissions, and ED visits for diabetes) showed an increase rather than an expected decrease in utilization (Revere et al., 2020).
The following (Assessment 9) evaluates whether the Texas DSRIP program meets the intention of the Triple Aim framework.
Assessment 9. Evaluation of the Texas DSRIP Program (Revere et al., 2020)
| # | Criteria | Evaluation |
|---|---|---|
| 1 |
Was the policy designed to achieve the intention of the Triple Aim framework? Evaluate the program’s success in: 1. Improvement in patient care experience |
This program was designed from the outset to achieve the intention of the Triple Aim. In their evaluation of the Texas Medicaid waiver program from 2011 through 2018, Revere and colleagues (2020) found the program to have shown positive, measurable results across two of three objectives (i.e., improvement in population health and enhancing the patient care experience) for the MLIU population in Texas. When using utilization as a proxy for cost, DSRIP 2.0 increased health care resource utilization. |
2.2 Be rooted in patient-centered value (Institute of Medicine, 2011)
Supporting Detail
Policymakers should design the health care system to maximize the value per dollar spent on the patient. The Institute of Medicine defines patient-centered care as “providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions” (Institute of Medicine, 2011). Patient-centered care involves all aspects of the health care system, from assessing value and determining coverage policies to care delivery. Health care reform should encourage the adoption of patient-centered care.
How to Use This Guiding Principle
Every policy reform initiative to moderate health care spending should be rooted in patient-centered value. For instance, patient-centered reforms should involve listening to patients and their family members and/or caregivers to define successful outcomes from the perspective of patients. Reviewers should evaluate policies to determine the extent that they move the system closer to or further away from a patient-centered health care system. For example, reviewers should examine the potential effects of implementing the policy on patients’ and caregivers’ health, out-of-pocket medical and nonmedical spending, and the patients’ and caregivers’ abilities to work or study.
Illustrative Example
The American College of Physicians defines Patient-Centered Medical Home (PCMH) as “a care delivery model where treatment is coordinated through their primary care physician to ensure they receive the necessary care when and where they need it, in a manner they can understand” (American College of Physicians, 2021). Centralized coordination that facilitates partnerships among patients, physicians and patients’ families may help with early diagnosis and treatment of comorbidities and potentially reduce the costs of uncoordinated care, such as duplicative procedures.
Crits-Christoph and colleagues (2018) examined how Pennsylvania’s Chronic Care Initiative (CCI), a statewide PCMH initiative implemented from 2008 to 2011, affected health care utilization and costs among HIV-positive Medicaid patients with comorbidities. The study compared health care utilization associated with patients treated in CCI practices and elsewhere using a claims database.
Crits-Cristoph and colleagues found that the CCI group experienced a statistically significant reduction in inpatient services, whereas the non-CCI group had increased inpatient claims. On the other hand, the study found an increase in outpatient care and pharmacy utilization for CCI patients compared with non-CCI patients (increase of 11.7% and 8.0% in the average number of claims per month, respectively).
The following (Assessment 10) evaluates whether the CCI program in Pennsylvania is grounded in patient-centered care.
Assessment 10. Evaluation of the CCI Program in Pennsylvania (Crits-Christoph et al., 2018)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the policy positively impact short- and long-term patient health (including caregiver impact)? | The authors found that the CCI program positively impacted short-term patient health. Specifically, patients in the CCI group experienced a significant reduction in inpatient services. They concluded that the CCI intervention appeared to shift inpatient costs and utilization to outpatient care and use of non-HIV medications. The impact on long-term outcomes was not clear. |
| 2 |
Did the policy enable care that is respectful of and responsive to individual patient preferences, needs and values, including:
|
The goal of the PMCH is to ensure patients receive the necessary care when and where they need it in a manner they can understand. The extent that Pennsylvania’s CCI program provided this care in a patient-centered manner is not clear. |
| 3 | How did the policy impact patient access to care, including nonmedical spending? | The goal of the PMCH is to ensure that patients receive necessary care where and when they need it. Patient outcomes improved, suggesting positive impacts on access to care. |
2.3 Recognize the differing needs of a diverse U.S. population (The National Health Council, 2019)
Supporting Detail
The U.S. health care system treats a diverse set of patients, differing in multiple ways — from their underlying biology and associated treatment response (heterogeneity of treatment effect) to their preferences and priorities (The National Health Council, 2019). Heterogeneity of treatment effect (e.g., efficacy and adverse events) can occur in members of the same family and across ethnic or socioeconomic groups. Similarly, differences in preferences and priorities (e.g., for survival or quality of life) may be observed among patients and providers and between provider and patient. Health care reform initiatives should respect and support the disparate needs of a diverse population.
How to Use This Guiding Principle
Reviewers should evaluate each policy to determine how it supports the needs of a diverse U.S. population. Not every individual policy can address the diverse needs of the U.S. population. However, health care spending policy should include targeted approaches to address the unique needs of specific populations. If reform does not support the needs of a particular population, a strategy to mitigate the consequence to this population should be explored. At a minimum, policies should not reduce the capacity to support these varied needs.
Illustrative Example
Note: This example is not a commentary on the expansion of Medicare; instead, it uses the following expansion analysis of Medicare’s ability to meet the needs of a diverse population as an example of how to evaluate a policy.
Medicare is the largest purchaser of health care in the United States, serving millions of Americans with disabilities and those over age 65. Landers and colleagues analyzed the role of Medicare in increasing access to care for racial and ethnic minorities and decreasing inequality in health coverage over a period from when the program began in 1966 (Landers et al., 2020).
In this analysis, Landers and colleagues (2020) noted that research has shown disparities in access to quality care for insured minorities within the Medicare program remain today. For instance, among Medicare beneficiaries, Landers found that those older and from racial and ethnic minority backgrounds report worse health indicators and receive a lower quality of care than white Medicare beneficiaries. Within Medicare Advantage plans, a recent study found that racial and ethnic minority beneficiaries’ ratings of their experiences with the health care system and health care access were worse than or equal to the ratings reported by white beneficiaries.
Further, Medicare contains noncapped, OOP deductibles and coinsurance, as well as coverage gaps for dental, vision and long-term services and supports. People of color are less likely to have supplemental coverage for these gaps. Given such disparity among the Medicare population, the authors stressed that any novel program should address other causes of health disparities such as housing availability, neighborhood conditions, food insecurity and educational opportunities. In addition, the novel program should consider other measures of inequality such as diversity and inclusion training for health care professionals and investments that could diversify the supply of clinicians (Landers et al., 2020).
The authors noted that the Affordable Care Act contains requirements for collecting health care data for minority populations in federally supported health care programs, which the authors believed was key to reducing disparities.
The following (Assessment 11) evaluates how Medicare program expansion meets the needs of a diverse U.S. population.
Assessment 11. Evaluation of the U.S. Medicare Program and Expansion Proposal (Landers et al., 2020)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the policy have a non-uniform impact on health outcomes across the population? | Landers and colleagues found that disparities in access to quality care for insured minorities within the Medicare program remain. For instance, among Medicare beneficiaries, those who are older and are from racial and ethnic minority backgrounds report worse health indicators and receive a lower quality of care than white Medicare beneficiaries. |
| 2 | Did the policy enable care that is respectful of and responsive to diverse patient preferences, needs and values? | The study did not evaluate how well the Medicare program meets diverse needs but did suggest potential areas that could, including housing availability, neighborhood conditions, food insecurity and educational opportunities. |
| 3 | How did the policy impact patient access to care? Were some patient populations disadvantaged compared to others? | Patient financial burden and access were not uniform across patient populations. Medicare contains noncapped, OOP deductibles and coinsurance, as well as coverage gaps for dental, vision and long-term services and supports. People of color are less likely to have supplemental coverage for these gaps. |
| 4 | Did the policy reduce the capacity to support varied patient needs? | Not applicable. |
2.4 Preserve or improve short- and long-term patient outcomes (National Quality Forum, 2009)
Supporting Detail
Health care reform approaches developed without consideration of their impact on short- and long-term outcomes or benefits for different patients can lead to worse patient outcomes. Understanding potential changes in both short- and long-term patient outcomes requires evaluating how reform might affect care over the natural trajectory of different clinical conditions (National Quality Forum, 2009). Such considerations will better assess a patient’s remaining lifetime health status and health care costs. As defined by the National Quality Forum (2009), this natural trajectory runs from prevention in the at-risk population to evaluation, initial management and follow-up care. Health care reform should create cost savings by modifying patient care in a manner that preserves or improves both short- and long-term outcomes.
How to Use This Guiding Principle
Aligned with the goal of the Triple Aim framework discussed in guiding principle 2.1, policy reform should sustain or improve the patient experience and the population outcomes in an extended timeline. At a minimum, no patient-centered health care reform framework or specific health policy should negatively impact outcomes to reduce spending. In 2009, the National Quality Forum presented the patient-centered framework for evaluating the efficiency of the U.S. health care system. This framework provides a helpful construct for assessing the impact of policy on outcomes. Leveraging this framework, reviewers should evaluate policy impact on outcomes throughout the entire life cycle of health care. This evaluation includes: 1) preventing events in the at-risk population; 2) providing evaluation and initial management during the acute phase; 3) providing follow-up care during the recovery and stabilization phase, including the strategy to manage disability; and 4) preventing the next episode. This framework aims to incorporate all care required to restore patients’ long-term quality of life and functional status. The framework demonstrates the relationships between preventive care, treatment for the acute event and long-term follow-up care (National Quality Forum, 2009).
Illustrative Example
In 2011, the Centers for Medicare and Medicaid Services (CMS) introduced Bundled Payments for Care Improvement (BPCI) to reduce the total cost of an episode of care while maintaining or improving the quality of care. The BPCI sought to minimize costs by bundling together payments based on historical Medicare billing for hospital and post-hospital care. Participants chose from three payment models, 48 clinical episodes, three episode lengths and three risk tracks.
Bundled payments may lead to unintended consequences, like underutilization for the sickest patients, later exacerbating the condition. So, while a bundled payment model may achieve positive short-term results in terms of cost, it may also produce adverse outcomes in the long term (e.g., increase in re-admissions) (LaPointe, 2020; Hardin et al., 2017).
CMS published the final BPCI evaluation for the entire five-year performance period of the initiative, from October 2013 through September 2018. The assessment includes Medicare claims-based impact estimates for key outcomes for Models 2, 3 and 4 and estimated savings to the Medicare program over the entire five years of the initiative (The Lewin Group, 2021).
“Consistent with previous reports, BPCI participants responded to the initiative’s incentives by reducing Medicare FFS payments. We continue to see this result from general patterns of reduced utilization and intensity of Post-Acute Care (PAC) use, with reductions in institutional care and decreases in the number of Skilled Nursing Facility (SNF) days among patients who receive SNF care. This decline did not translate into overall savings to Medicare after taking into account reconciliation payments made to participants. There are few indications in claims-based results that BPCI affected quality of care. However, three out of the 11 Model 3 SNF clinical episodes analyzed had an increase in readmissions, E.D. use, or mortality, potentially indicating a decrease in quality. However, these three clinical episodes suffer from small sample sizes, both overall and per SNF, making it difficult to ascertain whether these results are a signal or simply noise.
This final report shows differences in findings between surgical and medical clinical episodes. Under Model 2 hospitals, relative declines in total payments and payments for SNF, inpatient rehabilitation facility (IRF), and readmissions were similar for surgical and medical clinical episodes. Under Model 2 Physician Group Practices (PGP)s, relative declines in total payments, as well as SNF, IRF and HHA payments, were larger for surgical clinical episodes than medical clinical episodes. With respect to the effect of BPCI on quality of care as measured by readmissions, E.D. use, and mortality, there were no changes for Model 2 hospital-initiated episodes, and while there were a few indications of change for Model 2 PGP-initiated episodes, the direction was not consistent.
Results in the Year 5 Evaluation & Monitoring Annual Report also indicated that changes in functional status did not differ between beneficiaries in BPCI episodes and comparison beneficiaries, based on survey results, although fewer BPCI beneficiary respondents reported the highest level of satisfaction with their care. Quality of care was also maintained among vulnerable populations, including populations dually eligible for Medicare and Medicaid, with dementia, or with recent institutional PAC use (The Lewin Group, 2021).”
The following (Assessment 12) evaluates how BPCI impacted short- and long-term patient outcomes.
Assessment 12. Evaluation of the Bundled Payments for Care Improvement (The Lewin Group, 2021)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | What impact does the policy have on short-term patient outcomes? Relevant short-term outcomes include prevention, initial evaluation and treatment, and follow-up care. | There are few indications in claims-based results that BPCI affected quality of care. The instances of outcome changes were likely due to the small sample size. In addition, functional status was unchanged when compared to the status group. However, fewer beneficiaries report the highest level of satisfaction with care under the BCPI program. |
| 2 | What impact does the policy have on long-term patient outcomes? Long-term outcomes include the ability of care to restore patients’ long-term quality of life and functional status. | The study did not report impacts on long-term outcomes. |
2.5 Address the burden associated with the financing of health care and the resultant distributional consequences (Baicker, 2019)
Supporting Detail
Increasing total health care spending will require additional funding via higher premiums, higher patient out-of-pocket (OOP) costs, increased tax burden, and/or government funding diverted from other public services such as education and infrastructure. In some instances, these spending increases may be justified by the value of the care provided or be offset by increases in other areas of the economy; in other instances, this is not true. When the value of care is not high, and other gains do not offset spending increases, rising premiums and high patient OOP costs (in the form of high-deductible health plans, coinsurance and high max OOP caps) often result in consumers and patients losing insurance or being underinsured. Increasing taxes or shifting funding from other public services has consequences for the broader public and the economy. These effects are often not uniformly experienced within and outside the health system; instead, the consequences of these resultant distributional effects are often disproportionately worse for patients with lower socioeconomic status, thus creating significant disparities (Baicker, 2019).
How to Use This Guiding Principle
Individual policies to improve health outcomes may result in unintended negative consequences, such as increased disparities and reduced public services, due to health care spending changes. Therefore, reviewers should evaluate the distributional impacts, such as disparities and broader economic burden, resulting from proposed health care spending changes. This examination should identify potential sources of increased disparities, including higher premiums, higher patient OOP costs, increased tax burden, or government funding diverted from other public services such as education and infrastructure.
Illustrative Example
California’s laws and regulations create an effective budget cap for public expenditures. To assess the consequences of this public expenditure budget cap on individuals relying on public spending, Tran et al. (2017) used 25 years of General Fund expenditure data from California to estimate the effects of rapidly increasing health care spending on nonmedical social spending for tobacco control activities, restoring and expanding the number of high school counselors, and increasing the number of state preschool slots.
The authors found that while health care spending for Medicaid and other medical benefits increased over the 25 years from 14.1% to 21.3% of the General Fund expenditure, spending on public health and social programs fell from 34.8% in fiscal year 1990 to 21.4% in fiscal year 2014. The health care spending increase was associated with a 5.3-year gain in life expectancy between 1985 and 2010 in California, compared with an average improvement in the U.S. of 3.9 years during the same period. However, the authors suggested that reallocating ineffective medical care spending (assumed to be 21% of medical care spending) to cost-effective nonmedical social spending could have either prevented 10,500 premature deaths annually or helped an additional 418,000 high school students to graduate. The authors recognized that reallocation from inefficient care to nonmedical social spending interventions would not be simple to implement. Consequently, any estimates of the benefits from nonmedical social spending were subject to uncertainty.
The following (Assessment 13) evaluates the distributional consequences resulting from the interaction between California’s effective budget cap on public spending and increasing health care spending.
Assessment 13. Evaluation of California Budget Cap for Public Expenditures and Rising Health Spending (Tran et al., 2017)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Does the policy create higher premiums, higher patient OOP costs (in the form of high-deductible health plans, coinsurance, high max OOP caps), increased tax burden, or divert government funding from other public services? | Tran et al. (2017) stated that California’s laws and regulations create an effective budget cap on public spending, which led to decreased nonmedical social spending because of increased spending on Medicaid and other medical expenditures. |
| 2 | Does the proposed policy have positive or negative consequences for the broader public and economy? This evaluation includes the worsening of disparities. | Tran et al. (2017) estimated that 21% of increased health care spending was on ineffective care. The combination of the increased health spending and budget cap prevented this 21% from being spent on other public services. The authors estimate that these funds could have either prevented 10,500 premature deaths annually or helped an additional 418,000 high school students graduate. |
2.6 Target significant sources of inefficient health care spending across health care settings, services provided and differing conditions (VBID Health, 2017)
Supporting Detail
An efficient health care system can appropriately assess and reduce opportunity costs, which are defined as the loss in patient health outcomes attributable to spending on wasteful, inefficient and low-value care that reduces the funds available for high-value care. Analysis has shown that opportunity costs exist throughout the entire U.S. health care system (VBID Health, 2017). Therefore, improving the value of health care spending requires understanding significant sources of inefficiency across settings of care (outpatient and inpatient), services (procedures, drugs, diagnostics, devices, screenings), and stakeholder types (patients, payers, providers, manufacturers) (Cylus et al., 2016).
How to Use This Guiding Principle
Overall, health care reform approaches should focus on identifying and eliminating significant sources of inefficient care across the entire health system. However, no single policy will target all important sources of inefficient care; instead, individual policies should improve or, at a minimum, maintain the current efficiency level. Therefore, reviewers should evaluate individual policies to determine whether they improve or, at a minimum, maintain the current efficiency level.
Illustrative Example
The Choosing Wisely campaign is a nationwide initiative by the American Board of Internal Medicine Foundation to promote conversations between physicians and patients to make intelligent, effective health care choices that lead to high-quality care. The Washington State Alliance conducted a campaign in support of this initiative in Washington state. The campaign was developed using a Milliman MedInsight Health Waste Calculator analysis of the All-Payer Database in Washington state from January 1, 2014, to December 31, 2017. The analysis examined 47 of 48 of the calculator measures of tests, procedures and treatments known to be overused in both the commercially insured and Medicaid populations. On average, 846,973 individuals received services each year that were considered to be low value. The net result was $703 million spent on low-value care over the four years. Almost all of the wasted expenditure was driven by 11 of 47 low-value care practices identified.
Results of the analysis were made available to key stakeholders throughout the state as part of its Choosing Wisely campaign. In addition, the Washington Health Initiative proposed several actions to reduce this wasteful spending on both the demand side and the supply side of care. For example, officials recommended that clinicians “incorporate the reduction of overuse into local practice culture.” The result was a 10% decrease in low-value care in the commercially insured population and a 24% decrease in the Medicaid population (Washington Health Initiative, 2019).
The following (Assessment 14) summarizes how the study reviewed sources of inefficient health care spending.
Assessment 14. Evaluation of Washington State’s Choosing Wisely Campaign (Washington Health Initiative, 2019)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Does the policy improve or, at a minimum, maintain the current efficiency? | During the Choosing Wisely campaign, Washington state experienced a 10% and 24% decline in the use of low-value care in the commercially insured and Medicaid populations, respectively, over four years of reported data. |
| 2 | Is the policy part of a broader reform effort to address significant sources of inefficient care practices across conditions, services and stakeholder types? | The Washington Health Initiative focused on the use of low-value services across 47 care practices and conditions identified in the Choosing Wisely initiative. The focus of this effort spanned tests, procedures and medications. In addition, the effort spanned settings of care from inpatient to important ambulatory settings. |
2.7 Discourage the use of low-value care and encourage the use of high-value (VBID Health, 2017) care
Supporting Detail
The value delivered by the health care system is not uniform across interventions, diseases or populations. This variation exists for many reasons, such as different outcomes associated with different interventions for different populations; different condition characteristics by population, like disease severity; the level of disease-specific treatment innovation; the level of access to treatments; and other factors. Patient care is considered low value when it is wasteful, inefficient or the benefits don’t justify the costs or risks. Conversely, high-value care is when the benefits are high relative to the costs and risks. Health care reforms should recognize this inherent variation and seek to encourage the use of high-value treatments and discourage the use of low-value treatments (VBID Health, 2017).
How to Use This Guiding Principle
The health care system should be designed to spend dollars to maximize value for the patient. Therefore, health care reform initiatives should incorporate incentives, such as coverage policies and patient out-of-pocket costs, that encourage high-value care and discourage low-value care (Institute of Medicine, 2010). Reviewers should evaluate each new policy to determine whether it encourages high-value care or discourages low-value care. At a minimum, new policies should not discourage high-value care or incentivize low-value care.
Illustrative Example
Value-based insurance design (VBID) is a demand-side approach to health policy reform, aiming to increase health care quality and decrease costs by using financial incentives that promote cost-efficient health care services and consumer choices. Richardson and colleagues (2019) examined the VBID-X benefit model in a health care plan designed to bring the VBID model to the consumer insurance and exchange market by reducing or eliminating cost-sharing for a select set of high-value drugs and services, such as low-density lipoprotein testing, and increasing cost-sharing for low-value drugs and services, such as high-cost imaging (Richardson et al., 2017). Reductions in cost-sharing for high-value services varied. The cost-sharing for low-value care services was increased to offset reduced high-value service cost-sharing.
The targeted approach aims to avoid increases in premiums and deductibles while staying cost-neutral; the authors cited a recent survey conducted by the Kaiser Family Foundation reporting that 75% of individuals with chronic conditions and high deductibles skipped or delayed care. The authors concluded that VBID-X designs explicitly recognize the possibility of increasing accessibility to services deemed to improve patient-centered outcomes without increasing total health care costs.
The following (Assessment 15) summarizes how the policy achieved discouraging use of low-value treatments and encouraging use of high-value treatments.
Assessment 15. Evaluation of the VBID-X Benefit Model Design (Richardson et al., 2019)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Did the policy encourage the use of high-value care and discourage the use of low-value care to maximize value? If not, did the policy remain neutral with regard to low- and high-value services? | The VBID-X program was modeled to incentivize patients to shift their use of low-value services to high-value services and medications. The program achieves this goal by reducing copays and cost-sharing for high-value care and vice versa for low-value care. As a result, VBID-X remains cost-neutral while improving patient-centered outcomes. |
2.8 Address factors driving overall health care demand, including behavioral, cultural and socioeconomic factors (Adler and Prather, 2015; Artiga and Hinton, 2018)
Supporting Detail
Beyond a patient’s underlying biology, factors that drive demand for health care services include behavioral (e.g., smoking, diet), cultural (e.g., diet, views toward health system) and social determinants of health (Adler and Prather, 2015; Artiga and Hinton, 2018). Per the Centers for Disease Control and Prevention (CDC), “social determinants of health include aspects of the social environment (e.g., discrimination, income, education level, marital status), the physical environment (e.g., place of residence, crowding conditions, built environment [i.e., buildings, spaces, transportation systems, and products that are created or modified by people]), and health services (e.g., access to and quality of care, insurance status)” (CDC, 2010). These effects are often not uniformly experienced within and outside the health system; instead, the consequences of these resultant distributional effects are often disproportionately worse for patients with lower socioeconomic status, thus creating significant disparities (Baicker, 2019). Therefore, health care reform approaches should address the barriers created by these underlying factors to the extent that it is possible to change them.
How to Use This Guiding Principle
State, federal, and commercial initiatives that address rising health care spending should consider behavioral, cultural and socioeconomic factors contributing to higher health care spending. For example, health care reform approaches should include (1) incentives that encourage healthy behaviors linked to reduced health care spending and (2) initiatives to reduce cultural barriers that may prevent patients from accessing high-value care. Overall reform approaches should directly address these critical drivers of health care demand. In addition, when a policy targets a population with significant behavioral, cultural and socioeconomic factors, those factors must be considered. Otherwise, the policy may be less successful.
Illustrative Example
The Affordable Care Act included a federal mandate requiring restaurant chains with more than 20 locations to report the calories of items on their menus or menu boards. This requirement was designed to change eating behaviors that contribute to the high rate of obesity in the U.S. (35% of the population in 2011-2012). There is evidence that overweight individuals have an increased risk for many health conditions, including type 2 diabetes, heart disease, stroke and some cancers. Overweight individuals also have an estimated 42% higher annual cost of medical care than individuals of average weight.
Before this national mandate to report calorie information was implemented, the requirement was introduced in New York City in 2008. Following the New York City requirement, two studies (surveys of awareness and cash register receipts) attempted to determine whether customers at fast-food restaurants were aware of the calorie information and whether this information influenced the number of calories purchased from the restaurant (Elbel et al., 2009; Cantor et al., 2015).
Both studies showed that consumers were aware of the information and claimed to use the information, although awareness and use declined during the interval between the two studies. However, both studies showed that there were no statistically significant changes in levels of calories or nutrients purchased in restaurants displaying calorie information on their menus. In addition, the second study showed that there was no decrease in the frequency of visits to the fast-food chain restaurants with menu labeling. Thus, the authors of the second study concluded that “Menu labeling at fast-food chain restaurants, which the Affordable Care Act requires to be implemented nationwide in 2016, remains an unproven strategy for improving the nutritional quality of consumer food choices at the population level. Additional policy efforts that go beyond labeling and possibly alter labeling to increase its impact must be considered.”
The following (Assessment 16) summarizes how the study addressed factors driving overall health care demand, including behavioral, cultural and socioeconomic factors.
Assessment 16. Evaluation of the Federal Mandate for Calorie Reporting on Fast-Food Chain Restaurant Menus (Elbel et al., 2009; Cantor et al., 2015)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Does the overall reform approach address behavioral, cultural and socioeconomic factors contributing to rising health care spending? | This policy directly attempted to address the behavioral factors behind the U.S. obesity epidemic by requiring that restaurants with more than 20 sites provide caloric information on the menu. While the policy’s intention aligns with this guiding principle, the above study found that caloric information did not result in measurable changes in visits to or choices at fast-food chain restaurants. |
| 2 | When the policy is not explicitly focused on behavioral, cultural and socioeconomic factors contributing to rising health care spending, does the policy target a population with significant cultural and socioeconomic factors? If so, how has the policy addressed those considerations? | Not applicable (this policy focused explicitly on behavioral factors). |
2.9 Address misaligned incentives that distort utilization and price (Peter G. Peterson Foundation, 2020; American College of Physicians, 2009)
Supporting Detail
Misaligned incentives within the U.S. health care system play a key role in driving health care services’ utilization and pricing. This effect can be negative by creating and promoting low-value care. Sources of misaligned incentives can include reimbursement policy, competition, regulation, malpractice laws and tax policy (Peter G. Peterson Foundation, 2020; American College of Physicians, 2009). Examples of these misaligned incentives impacting price and utilization exist throughout the health care system. For example, patients may not receive high-value health care services due to reimbursement policies that restrict provider or site-of-care options. Another example is the tax incentive for selecting generous employment-based health benefits for highly paid individuals, leading to the overconsumption of low-value medical care. In a third example, when various regulations and tax policies influence consolidations in the health care market, limited competition may lead to higher health care prices. Finally, a fragmented health care system may result in inefficient care coordination due to more administrative complexities. Therefore, the overall health care reform approach needs to identify and address the most critical structural deficiencies.
How to Use This Guiding Principle
State, federal or commercial reform initiatives targeting rising health care spending should address misaligned incentives contributing to wasteful spending and higher prices for health care services. Such policies should include active monitoring strategies to identify unintended consequences as they emerge. Misaligned incentives are not expected to be the focus of every individual policy. However, each new policy should be evaluated to determine whether it creates additional price and/ or utilization distortions.
Illustrative Example
The Affordable Care Act included a proposal to levy an excise tax on high-cost health insurance plans (known as the Cadillac tax). The aim was to help fund the extended health care coverage under Medicaid expansion and control rising health care costs. A study by Warshawsky and Leahy (2018), using National Compensation Survey data to analyze who would be impacted by this tax, estimated that between 11% and 12% of workers participating in employer-provided health plans in 2020 would be subject to this tax. The authors further estimated that the percentage of workers would rise to approximately 25% by 2025 (Warshawsky and Leahy, 2018). The percentages of workers subject to this tax would vary by worker characteristics (region, number of employees at the company, unionization, industry and occupation). The authors concluded, “Economic theory would predict that employees and employers will substitute away from high premium plans and toward plans with higher deductibles and lower premiums. In addition, firms’ attempts to reduce their overall tax burden should lead to tighter negotiations with providers and, eventually, to more serious engagement by employers, employees, and insurers in managing health plans and reducing costs.” However, the authors did not cite any studies supporting these assumptions (Warshawsky and Leahy, 2018).
The following (Assessment 17) summarizes how the study addressed structural deficiencies that may distort utilization and price.
Assessment 17. Evaluation of the Excise Tax on High-Cost Health Insurance Plans (Warshawsky and Leahy, 2018)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Does the overall reform approach address misaligned incentives contributing to wasteful spending and higher prices for health care services? | The Cadillac tax was intended to address the structural distortions resulting from the tax subsidization of highcost employer health plans. Warshawsky and Leahy (2018) estimated that 25% of employees would be impacted by 2025. The authors speculate that the increased tax pressure would drive employers and employees to lower-cost plans with higher deductibles. |
| 2 | Does the reform approach include active monitoring of potential impacts? | Not applicable (the policy was repealed and never implemented). |
| 3 | When the policy is not targeting misaligned incentives, does the policy introduce new utilization or price distortions? | If implemented, the Cadillac tax may have harmed patients with employer plans by accelerating the market trend of increasing deductibles and out-of-pocket costs (Dorn, 2019). |
2.10 Incentivize innovations in health care delivery systems and treatments (Institute of Medicine, 2013; McClellan et al., 2017)
Supporting Detail
Continuing innovations in health care delivery systems and treatments are critical to address inefficiencies in the current system and improve patient outcomes in many acute and chronic diseases. Health care spending policies should provide incentives to payers, providers and developers to improve system efficiency or provide high-value care that improves patient health outcomes. Where possible, such policies should avoid creating disincentives (Institute of Medicine, 2013).
How to Use This Guiding Principle
Policy reforms to moderate health care spending should consider the potential consequences of the overall initiative on innovations in health care delivery systems and treatments. As such, reviewers should evaluate policies for impacts on innovation incentives and potential consequences for patients.
Illustrative Example
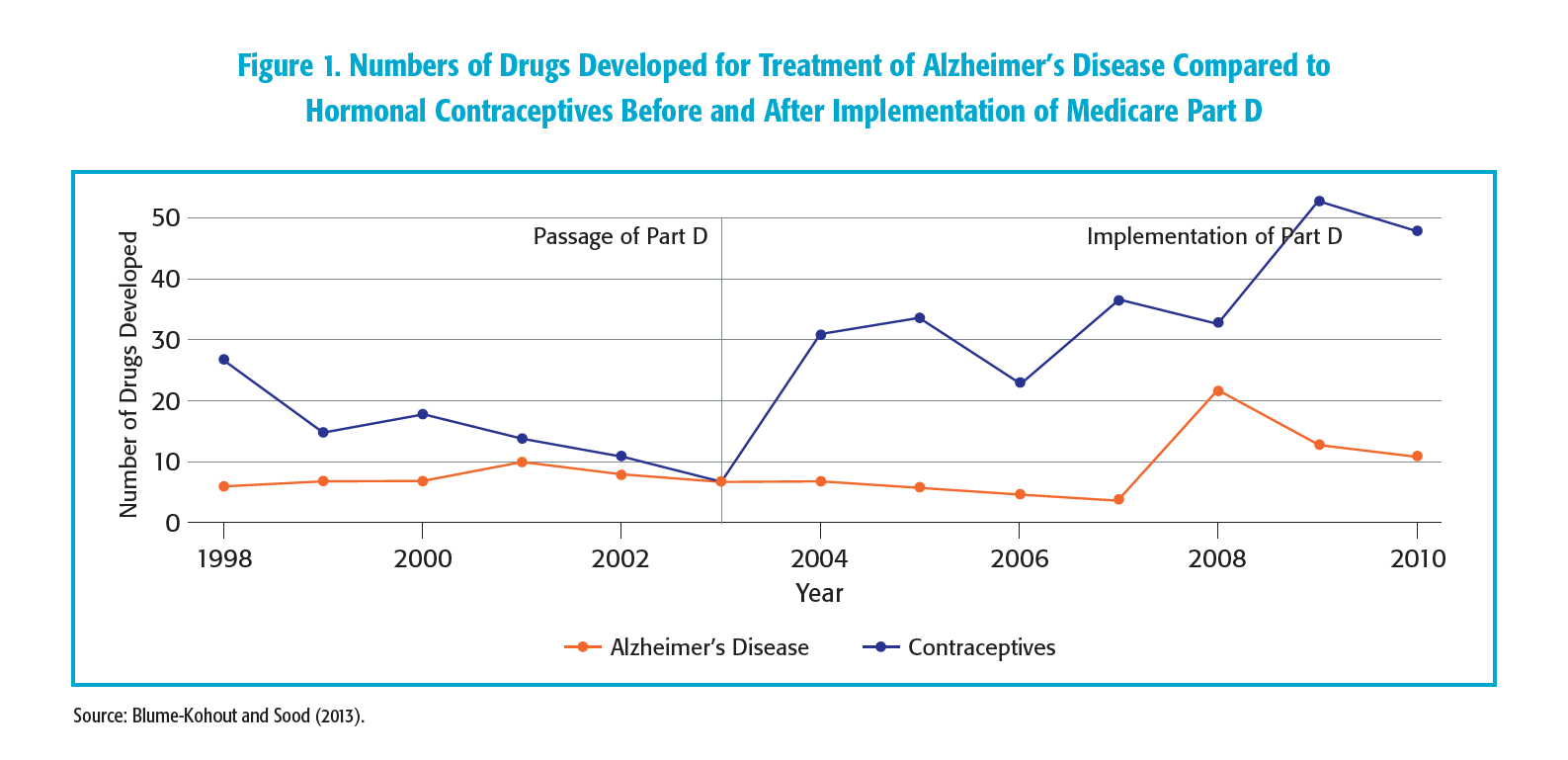
The Medicare prescription drug benefit (Medicare Part D) is an optional federal program covering self-administered prescription drugs among Medicare beneficiaries. The program was implemented in 2006 and was followed by an increase in self-administered prescription drugs among seniors. Blume-Kohout and Sood (2013) assessed the positive impact of Medicare Part D on pharmaceutical research and development by using time-series data on the number of drugs entering preclinical and clinical development, categorized by therapeutic class and phase. The authors found that the passage and implementation of Medicare Part D was associated with significant increases in pharmaceutical research and development activities for therapeutic classes with higher Medicare market shares. Figure 1 presents a comparison of the research and development activities for drugs developed between 1998 and 2010 for treatments for Alzheimer’s disease compared to drugs developed in the same period for hormonal contraception (Blume-Kohout and Sood, 2013).
The following (Assessment 18) summarizes how this example addressed the reward for long-term innovation in health care delivery systems and treatments.
Assessment 18. Evaluation of the Impact of Medicare Part D on Long-Term Innovations and Population Health Outcomes (Blume-Kohout and Sood, 2013)
| # | Criteria | Evaluation |
|---|---|---|
| 1 | Does the policy affect innovations in health care delivery systems and treatments? | Blume-Kohout and Sood (2013) found that the passage and implementation of Medicare Part D was associated with significant increases in pharmaceutical research and development activities for therapeutic classes with higher Medicare market shares. Specifically, the authors found that the number of drugs entering phase 1 trials after the passage of Part D more than doubled for antipsychotic, antidepressant, and gastrointestinal ulcer treatments, even though the success rate for these drugs before phase 3 trials appears to have been low. While the authors found a correlation between passage of Part D and innovation, they did not establish causality. |
| 2 | Do the changes in incentives impact population health outcomes? | Blume-Kohout and Sood (2013) did not estimate the impact of Medicare Part D on population health outcomes. |
References
Adler NE, Prather AA. 2015. “Determinants of Health and Longevity.” Population Health: Behavioral and Social Science Insights. Rockville, MD: Agency for Health Care Research and Quality. Available at http://www.ahrq.gov/professionals/education/curriculum-tools/population-health/adler.html. Accessed July 7, 2020.
American College of Physicians. 2009. “Controlling Health Care Costs While Promoting the Best Possible Health Outcomes.” Available at https://www.acponline.org/acp_policy/policies/controlling_healthcare_costs_2009.pdf. Accessed August 3, 2020.
American College of Physicians. 2021. “What Is the Patient-Centered Medical Home?” Available at https://www.acponline.org/practice-resources/business-resources/payment/delivery-and-payment-models/patient-centered-medical-home/understanding-the-patient-centered-medical-home/what-is-the-patient-centered-medical-home. Accessed March 23, 2021.
Artiga S, Hinton E. 2018 (May 10). “Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity.” Available at https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/. Accessed August 3, 2020.
Baicker K. 2019. “Economic Analysis for Evidence-Based Health Policy: Progress and Pitfalls.” Natl Bureau Econ Res Report. 3:1-6.
Bisognano M, Kenney C. 2012. Pursuing the Triple Aim: Seven Innovators Show the Way to Better Care, Better Health, and Lower Costs. New York: John Wiley & Sons.
Bekemeier B, Yang Y, Dunbar MD, Pantazis A, Grembowski DE. 2014 (June). “Targeted Health Department Expenditures Benefit Birth Outcomes at the County Level.” Am J Prev Med. 46(6):569-77.
Blume-Kohout M, Sood N. 2013. “Market Size and Innovation: Effect of Medicare Part D on Pharmaceutical Research and Development.” J Public Econ. 97:327-36.
Cantor J, Torres A, Abrams C, Elbel B. 2015 (November). “Five Years Later: Awareness of New York City’s Calorie Labels Declined, with No Changes in Calories Purchased.” Health Aff (Millwood). 34(11):1893-900.
Centers for Disease Control and Prevention (CDC). 2010 (October). “Establishing a Holistic Framework to Reduce Inequities in HIV, Viral Hepatitis, STDs, and Tuberculosis in the United States.” Atlanta (GA): U.S. Department of Health and Human Services, CDC.
Centers for Medicare and Medicaid Services (CMS). 2017. “National Health Expenditure Accounts: Methodology Paper.” Available at https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/dsm-17.pdf. Accessed July 6, 2020.
Crits-Christoph P, Gallop R, Noll E, et al. 2018 (August). “Impact of a Medical Home Model on Costs and Utilization among Comorbid HIV-Positive Medicaid Patients.” Am J Manag Care. 24(8):368-75.
Cutler DM, Ghosh K, Messer KL, Raghunathan TE, Stewart ST, Rosen AB. 2019 (February). “Explaining the Slowdown in Medical Spending Growth Among the Elderly, 1999-2012.” Health Aff (Millwood). 38(2):222-9.
Cylus J, Papanicolas I, Smith PC. 2016. “A Framework for Thinking about Health System Efficiency.” Available at https://www.ncbi.nlm.nih.gov/books/NBK436891/. Accessed February 18, 2021.
Dieleman JL, Squires E, Bui AL, et al. 2017. “Factors Associated With Increases in U.S. Health Care Spending, 1996-2013.” JAMA. 318:1668-78.Dorn S. 2019 (June 18) “The Cadillac Tax: It’s Time To Kill This Policy Zombie.” Health Affairs blog. Available at https://www.healthaffairs.org/do/10.1377/hblog20190617.795057/full/.
Dunn A, Grosse SD, Zuvekas SH. 2018 (February). “Adjusting Health Expenditures for Inflation: A Review of Measures for Health Services Research in the United States.” Health Serv Res. 53(1):175-96.
Elbel B, Kersh R, Brescoll VL, Dixon LB. 2009 (November-December). “Calorie Labeling and Food Choices: A First Look at the Effects on Low-Income People in New York City.” Health Aff (Millwood). 28(6):w1110-21.
Hardin L, Kilian A, Murphy E. 2017. “Bundled Payments for Care Improvement Preparing for the Medical Diagnosis-Related Groups.” J Nurs Admin. 47(6):313-9.
Husereau D, Drummond M, Petrou S, et al. 2013. “Consolidated health economic evaluation reporting standards (CHEERS)—explanation and elaboration: a report of the ISPOR health economic evaluation publication guidelines good reporting practices task force.” Value in Health. 16.2: 231-250.
Hernandez I, San-Juan-Rodriguez A, Good CB, Gellad WF. 2020 (March 3) “Changes in List Prices, Net Prices, and Discounts for Branded Drugs in the U.S., 2007-2018.” JAMA. 323(9):854-62.
Institute of Medicine. 2010. “The Healthcare Imperative: Lowering Costs and Improving Outcomes: Workshop Series Summary.” Washington, DC: The National Academies Press. Available at https://doi.org/10.17226/12750.
Institute of Medicine. 2011. “Patients Charting the Course: Citizen Engagement and the Learning Health System: Workshop Summary.” Washington, DC: The National Academies Prehttps://doi.org/10.17226/13444ss. Available at https://doi.org/10.17226/12848. Accessed July 23, 2021.
Institute of Medicine. 2013. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Washington, DC: The National Academies Press. Available at https://doi.org/10.17226/13444.
IQVIA Institute for Human Data Science. 2021 (May). “The Use of Medicines in the U.S.: Spending and Usage Trends and Outlook to 2025.” Available at https://www.iqvia.com/insights/the-iqvia-institute/reports/the-use-of-medicines-in-the-us. Accessed June 28, 2021.
Irwin A, Jozaghi E, Weir VW, Allen ST, Lindsay A, Sherman SG. 2017 (May 12). “Mitigating the Heroin Crisis in Baltimore, MD, USA: A Cost-Benefit Analysis of a Hypothetical Supervised Injection Facility.” Harm Reduct J.14(1):29.
Landers RM, Vladeck B, Cole BK. 2020 (March 23). “Medicare’s Current and Future Role in Reducing Racial and Ethnic Health Disparities.” Health Affairs blog. Available at https://www.healthaffairs.org/do/10.1377/hblog20200319.932279/full/. Accessed March 22, 2021.
LaPointe J. 2020. “CMS Releases Initial Report on Risk-Based Bundled Payment Model.” Available at https://revcycleintelligence.com/news/cms-releases-initial-report-on-risk-based-bundled-payment-model. Accessed July 7, 2020.
McClellan MB, Feinberg DT, Bach PB, et al. 2017 (March 17). “Payment Reform for Better Value and Medical Innovation.” NAM Perspectives. Available at https://nam.edu/wp-content/uploads/2017/03/Payment-Reform-for-Better-Value-and-Medical-Innovation.pdf. Accessed February 22, 2021.
National Quality Forum. 2009. “Measurement Framework: Evaluating Efficiency Across Patient-Focused Episodes of Care [abstract].” Available at https://www.qualityforum.org/Publications/2010/01/Measurement_Framework__Evaluating_Efficiency_Across_Patient-Focused_Episodes_of_Care.aspx. Accessed July 7, 2020.
Peter G. Peterson Foundation. 2020 (April 20). “Why Are Americans Paying More for Health Care?” Available at https://www.pgpf.org/blog/2020/04/why-are-americans-paying-more-for-health care. Accessed August 3, 2020.
Revere L, Kavertapu N, Hall J, Begley C. 2020. “Achieving Triple Aim Outcomes: An Evaluation of the Texas Medicaid Waiver.” Inquiry. 57:0046958020923547.
Richardson H, Budros M, Chernew ME, Fendrick AM. 2019 (July 15). “V-BID X: Creating a Value-Based Insurance Design Plan for the Exchange Market.” Health Affairs blog. Available at https://www.healthaffairs.org/do/10.1377/hblog20190714.437267/full/. Accessed March 22, 2021.
Smith M, Lix LM, Azimaee M, Enns JE, Orr J, Hong S and Roos LL. 2018 (March 1). “Assessing the Quality of Administrative Data for Research: A Framework from the Manitoba Centre for Health Policy.” J Am Med Inform Assoc. 25(3):224-29.
The National Health Council. 2019 (June). “The National Health Council Rubric to Capture the Patient Voice: A Guide to Incorporating the Patient Voice into the Health Ecosystem.” Available at https://www.nationalhealthcouncil.org/Patient-Engagement-Rubric. Accessed August 4, 2020.
The Lewin Group. 2021 (March). “CMS Bundled Payments for Care Improvement Initiative Models 24: Year 7 Evaluation & Monitoring Annual Report.” Available at https://innovation.cms.gov/data-and-reports/2021/bpci-models2-4-yr7evalrpt. Accessed May 10, 2021.
Thorpe KE, Howard DH, Galactionova K. 2007 (November-December). “Differences in Disease Prevalence as a Source of the U.S.-European Health Care Spending Gap.” Health Aff (Millwood). 26(6):w678-86.
Tran LD, Zimmerman FJ, Fielding JE. 2017. “Public Health and the Economy Could Be Served by Reallocating Medical Expenditures to Social Programs.” SSM Popul Health. 3:185-91.
VBID Health. 2017. “Tackling the epidemic of low-value spending and medical overuse: opportunities for purchasers and carriers.” Available at http://www.vbidhealth.com/docs/TF-LVC-%20White%20Paper%20-%20October%20Draft.pdf. Accessed August 3, 2020.
Walker D, Fox-Rushby J. 2001 (December). “Allowing for Uncertainty in Economic Evaluations: Qualitative Sensitivity Analysis.” Health Policy Plan. 16(4):435-43.
Wamble D, Ciarametaro M, Houghton K, Ajmera M, Dubois RW. 2019 (January). “What’s Been the Bang for the Buck? Cost-Effectiveness of Health Care Spending Across Selected Conditions in the U.S.” Health Aff (Millwood). 1;38(1):68-75.
Washington Health Initiative. 2019 (October). “Right Care: First, Do No Harm: Calculating Health Care Waste in Washington State Multi-Year and Medical Group Results.” Available at https://www.wacommunitycheckup.org/media/47217/first-do-no-harm-oct-2019.pdf. Accessed June 10, 2021.
Warshawsky MJ, Leahy M. 2018 (April). “Affordable Care Act’s Cadillac Tax Could Affect One-Fourth of Workers With Employer Health Coverage by 2025.” Health Aff (Millwood). 37(4):613-18.
White C, Whaley CM. 2019. “Prices Paid to Hospitals by Private Health Plans Are High Relative to Medicare and Vary Widely: Findings From an Employer-Led Transparency Initiative.” Available at https://www.rand.org/pubs/research_reports/RR3033.html. Accessed August 3, 2020.
Wyatt R, Laderman M, Botwinick L, Mate K, Whittington J. 2016. “Achieving Health Equity: A Guide for Health Care Organizations.” Institute for Health Care Improvement. Available at http://www.ihi.org/resources/Pages/IHIWhitePapers/Achieving-Health-Equity.aspx. Accessed February 22, 2021.
Yoon J, Fonarow GC, Groeneveld PW, Teerlink JR, Whooley MA, Sahay A, Heidenreich PA. 2016. “Patient and Facility Variation in Costs of V.A. Heart Failure Patients.” JACC Heart Fail. 4(7):551-8.
These Patient-Centered Guiding Principles for Reforming Health Care to Address Rising Health Care Spending are one part of NPC's Health Care Spending Guiding Principles. Click here for the Patient-Centered Guiding Principles for Evaluating Health Care Spending.
Read the full Health Care Spending Guiding Principles
These principles are intended to guide a rigorous, evidence-based evaluation and discussion of health care spending estimates and policies. They aim to improve health care spending efficiency and maximize patient health.